Courtesy: Prof James Wittig
Orthopaedic Oncologist
Sarcoma Surgeon
www.tumorsurgery.org
James Wittig books
Radiolucent Bone Lesions: Structured Clinical Summary
Overview
- Radiolucent bone lesions appear as lytic areas without internal mineralization on imaging.
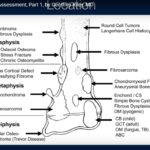
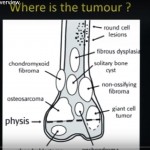
- Common entities include giant cell tumor, aneurysmal bone cyst, unicameral bone cyst, eosinophilic granuloma, and non ossifying fibroma.
- Clinical interpretation depends on patient age, lesion location, radiographic features, and histology.
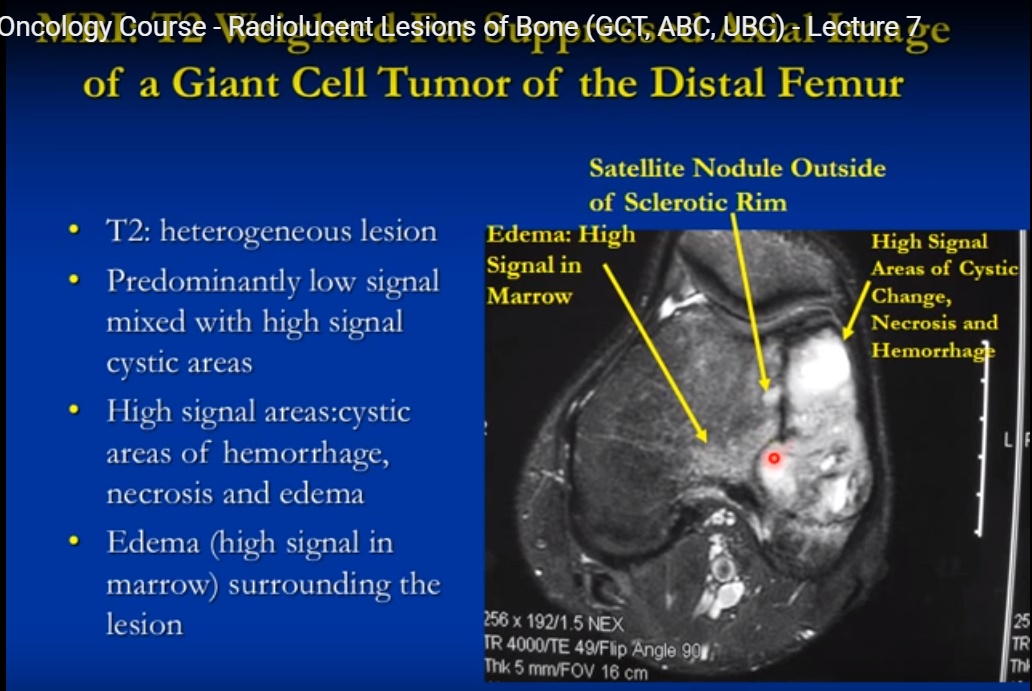
Giant Cell Tumor
- Benign but locally aggressive tumor composed of osteoclast like giant cells and mononuclear stromal cells.
- Typically affects skeletally mature individuals between 20 and 40 years.
- Common locations include distal femur, proximal tibia, distal radius, and sacrum.
- Radiographs show eccentric metaphyseal lesion extending into epiphysis without mineralization.
- Often lacks sclerotic margin and may demonstrate cortical thinning, expansion, or soft tissue extension with intact periosteum.
- Magnetic resonance imaging shows heterogeneous signal with cystic or hemorrhagic components.
- Treatment is intralesional curettage with adjuvant therapy and cement reconstruction; en bloc resection is reserved for advanced cases.
Aneurysmal Bone Cyst
- Benign aggressive lesion composed of blood filled cystic spaces separated by fibrous septa.
- Most common in children and adolescents and often arises in metaphysis of long bones.
- May occur secondary to other tumors such as chondroblastoma or giant cell tumor.
- Radiographs demonstrate expansile lytic lesion with cortical thinning and remodeling.
- Magnetic resonance imaging often shows multiple fluid fluid levels from hemorrhage.
- Treatment typically involves curettage and bone grafting; recurrence is relatively common.
Unicameral Bone Cyst
- Non neoplastic fluid filled cavity lined by thin fibrous membrane.
- Common in patients younger than 20 years, especially males.
- Typical sites include proximal humerus and proximal femur.
- Radiographs show central metaphyseal lesion with thin sclerotic rim and mild expansion.
- Fallen fragment sign may be present after pathological fracture.
- Management includes observation for asymptomatic cases or curettage, grafting, or steroid injection for symptomatic lesions.
Eosinophilic Granuloma
- Localized form of Langerhans cell histiocytosis involving bone.
- Occurs primarily in children between 5 and 15 years.
- Common sites include skull, mandible, ribs, pelvis, and long bones.
- Radiographic appearance varies from well defined lytic lesion to aggressive permeative pattern.
- May show vertebra plana when involving spine.
- Histology demonstrates Langerhans cells with grooved nuclei and inflammatory infiltrate.
- Treatment ranges from observation to curettage and grafting depending on symptoms.
Non Ossifying Fibroma
- Benign fibrous lesion arising from cortex and extending into medullary canal.
- Common incidental finding in adolescents and young adults.
- Most frequent in distal femur, proximal tibia, and distal tibia.
- Radiographs show eccentric metaphyseal lesion with thick sclerotic margin and lobulated contour.
- Usually asymptomatic and resolves spontaneously with skeletal maturity.
- Large symptomatic lesions may require curettage and bone grafting.
Key Imaging Considerations
- Radiolucent lesions lack calcified matrix and appear lytic on radiographs.
- Magnetic resonance imaging helps evaluate extent and soft tissue involvement.
- Bone scan uptake varies depending on lesion type and activity.
- Clinical context and biopsy are essential for definitive diagnosis.

Leave a Reply