Courtesy: Dr S Macdonald, Ashok Shyam TV, Ortho
Don’t Forget Pre-Operative Evaluation
Before analyzing a painful postoperative knee, always revisit:
-
Was TKA truly indicated?
-
Was there clear bone-on-bone osteoarthritis?
-
Could pain have originated elsewhere (e.g., hip)?
Key Clinical Lesson
-
Mild radiographic knee arthritis + severe hip arthritis ? knee replacement will not solve the pain.
-
Always evaluate:
-
Ipsilateral hip
-
Lumbar spine
-
Referred pain patterns
-
Inappropriate indication leads to persistent postoperative pain.
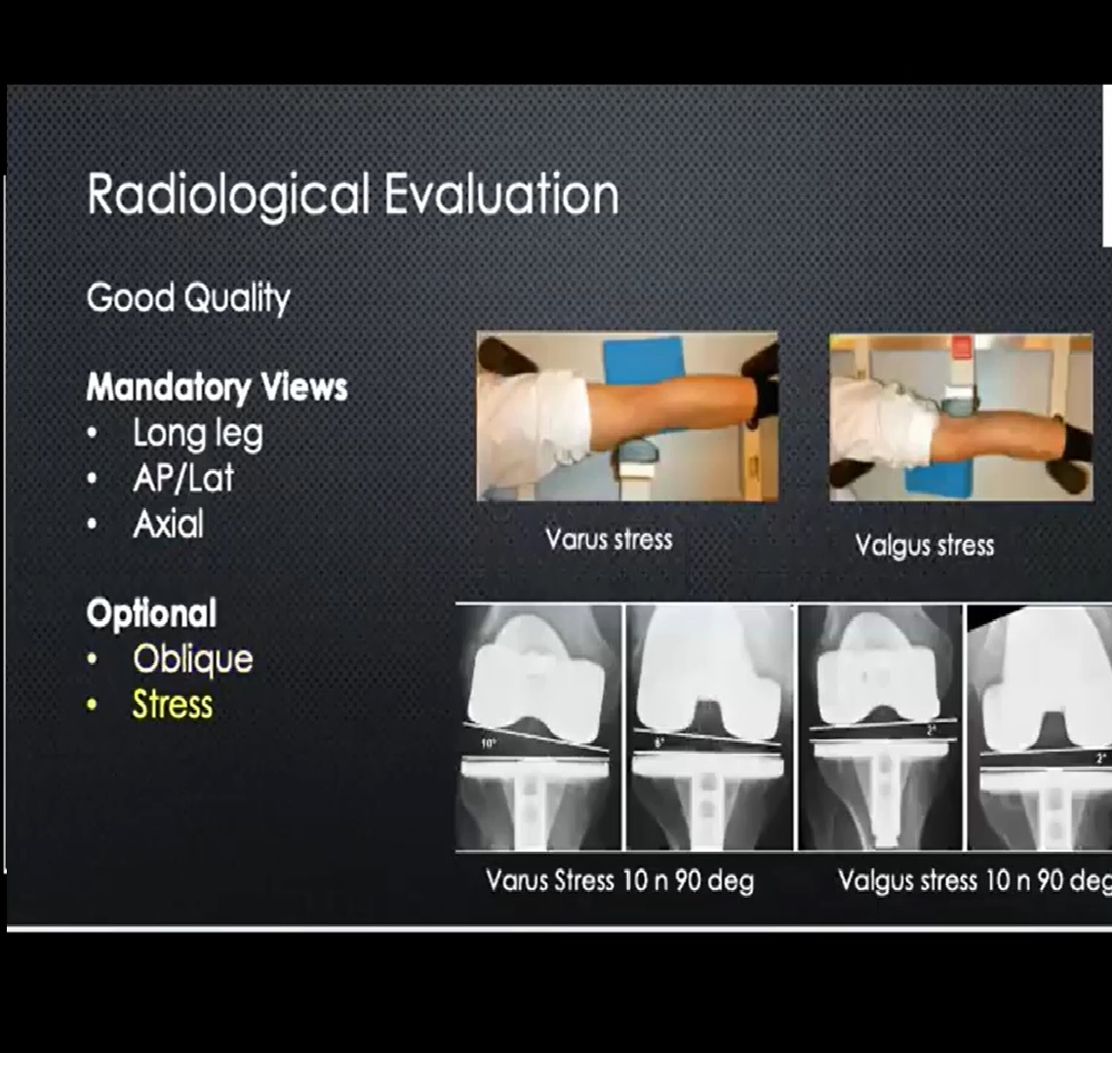
Postoperative Radiographic Assessment: Three Pillars
-
Limb Alignment
-
Balancing
-
Component Alignment & Orientation
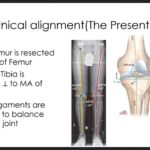
1?? Limb Alignment
Goal
-
Mechanical axis:
-
Center of hip ? center of knee ? center of ankle.
-
Does It Have to Be Perfect?
-
Traditional target: ±3° from neutral.
-
Long-term data (15-year follow-up studies):
-
No significant difference in function or survivorship between:
-
Knees within 3°
-
Knees outside 3°
-
-
Takeaway:
-
Aim for neutral.
-
Minor deviations may not compromise long-term results.
-
Avoid gross malalignment.
2?? Balancing
Even on early postoperative films, you can assess balance.
What to Look For
-
Symmetry between femoral component and polyethylene insert.
-
Medial and lateral compartment congruence.
Warning Signs
-
Lift-off on one side (especially medial side in former varus knees).
-
Asymmetric joint space.
Joint Line Elevation: Is It Always Bad?
Traditional teaching:
-
Elevation = poor function.
Evidence suggests:
-
Minor elevation (2–4 mm) does NOT necessarily:
-
Affect function.
-
Reduce survivorship.
-
Alter clinical outcomes.
-
Key principle:
-
Proper flexion–extension gap balance is more important than millimeter-perfect joint line restoration.
3?? Component Positioning
Malposition can cause:
-
Pain
-
Stiffness
-
Instability
-
Increased wear
-
Early failure
? Femoral Component
Sagittal Plane
Target:
-
Parallel to femoral shaft.
-
Flush with anterior cortex.
Common Errors
| Error | Consequence |
|---|---|
| Excessive flexion | Fixed flexion contracture, anterior pain |
| Excess anterior translation | Patellofemoral overstuffing |
| Notching | Fracture risk (large notch) |
| Excess posterior resection | Tight flexion gap |
Small notches may not be clinically significant.
Coronal Plane
-
5–7° valgus to anatomical axis.
-
Slightly central to lateral placement preferred.
Errors:
-
Excess valgus ? wear, pain.
-
Medial shift ? patellar instability.
Rotational Alignment (Most Critical)
Target:
-
~3° external rotation relative to posterior condylar axis.
Pitfall:
-
Valgus knees with hypoplastic lateral condyle.
-
Posterior referencing jigs may create internal rotation.
-
Leads to:
-
Patellar maltracking
-
Anterior knee pain
-
Stiffness
-
-
? Tibial Component
Coronal Alignment
-
90° to long axis of tibia.
Malalignment ? excessive polyethylene wear.
Tibial Slope
Debated topic:
-
CR knees: 3° posterior slope common.
-
PS knees: some prefer 0°, others still use slope.
Consequences:
| Error | Effect |
|---|---|
| Too much slope | Flexion instability |
| Too little slope | Tight flexion gap, stiffness (especially CR knees) |
Tibial Rotation
Target:
-
Medial one-third of tibial tubercle.
Malrotation leads to:
-
Patellar maltracking.
-
Patellar instability.
-
Anterior knee pain.
? Patellar Component
Target:
-
Central or slightly medial placement.
Common mistake:
-
Excess lateral placement ? instability.
Radiographic Clues to Common Clinical Problems
Stiff Knee
Look for:
-
Oversized components.
-
Overstuffed flexion gap.
-
Too little tibial slope (especially CR).
-
Tight flexion space.
Instability
Look for:
-
Undersized femoral component.
-
Loose flexion gap.
-
Excess tibial slope.
-
Asymmetric polyethylene thickness.
Persistent Pain
Look for:
-
Overhanging components.
-
Focal implant prominence.
-
Malrotation.
-
Joint line mismatch.
-
Patellofemoral overstuffing.
Always correlate imaging with clinical exam.
Final Clinical Pearls
-
Not every painful TKA is a technical failure.
-
Not every malalignment leads to failure.
-
Indication matters as much as execution.
-
Evaluate hip and spine in every painful knee.
-
Minor radiographic imperfections may be clinically irrelevant.
-
Major malrotation errors are rarely forgiving.


Leave a Reply