Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
GENERAL OVERVIEW
-
The radial nerve is the primary motor nerve of the posterior compartment of the arm and forearm.
-
It provides motor innervation to:
-
The triceps brachii muscle
-
The wrist and finger extensors
-
-
It also provides sensory innervation to a large portion of the dorsum of the hand.
COURSE IN THE ARM
-
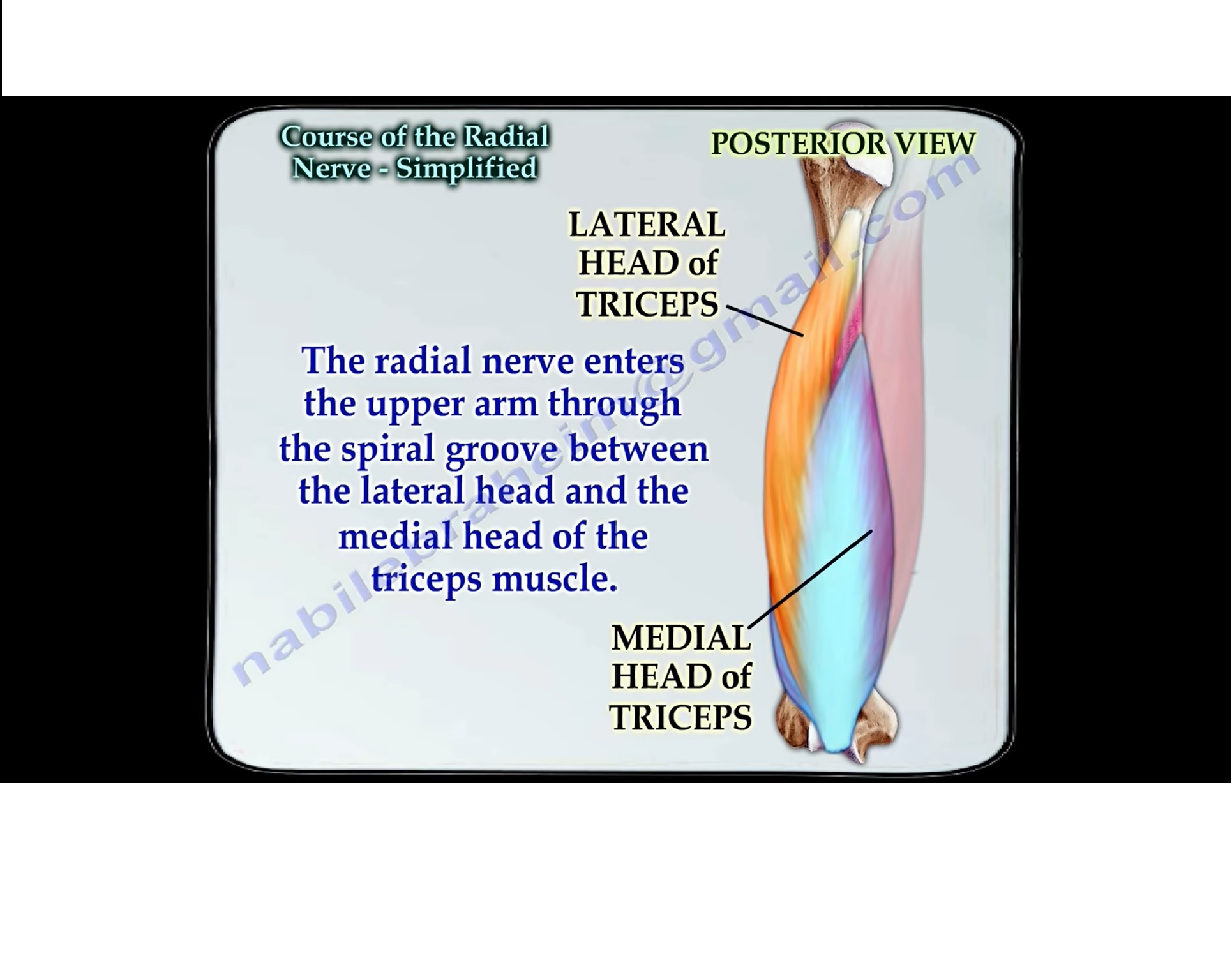
The radial nerve descends in the arm and enters the posterior compartment.
-
It passes through the spiral groove (radial groove) on the posterior aspect of the humerus.
-
In the spiral groove, it lies:
-
Between the medial head and lateral head of the triceps muscle
-
-
In this region, the nerve is particularly vulnerable in mid-shaft fractures of the humerus.
TRANSITION TO THE ANTERIOR ARM
-
After traversing the spiral groove, the radial nerve pierces the lateral intermuscular septum.
-
It enters the anterior compartment of the arm, just above the elbow.
-
In the distal arm, it supplies motor branches to:
-
Brachioradialis
-
Extensor carpi radialis longus
-
Extensor carpi radialis brevis
-
COURSE AT THE ELBOW
-
At the level of the elbow, the radial nerve divides into two terminal branches:
-
Posterior interosseous nerve (motor)
-
Superficial branch of the radial nerve (sensory)
-
POSTERIOR INTEROSSEOUS NERVE
-
The posterior interosseous nerve enters the forearm by passing through the supinator muscle.
-
It passes beneath a fibrous arch of the supinator known as the Arcade of Frohse, a common site of nerve compression.
-
After emerging from the supinator:
-
It enters the posterior compartment of the forearm.
-
Supplies the superficial extensor muscles, followed by the deep extensor muscles of the forearm.
-
-
It provides pure motor innervation and has no cutaneous sensory supply.
SUPERFICIAL BRANCH OF THE RADIAL NERVE
-
The superficial branch continues along the lateral aspect of the forearm.
-
It runs deep to the brachioradialis muscle.
-
Distally, it becomes subcutaneous and enters the hand.
-
It provides sensory innervation to:
-
The dorsum of the hand
-
The dorsal aspects of the radial digits (excluding nail beds)
-
CLINICAL CORRELATION
-
Injury at the spiral groove may cause:
-
Wrist drop
-
Loss of finger extension
-
Preserved elbow extension if triceps branches are spared
-
-
Compression at the Arcade of Frohse may result in:
-
Posterior interosseous nerve palsy
-
Motor weakness without sensory loss
-
-
Injury to the superficial branch leads to:
-
Sensory loss over the dorsum of the hand without motor deficit
-
KEY POINTS
-
The spiral groove is the most vulnerable segment of the radial nerve.
-
Posterior interosseous nerve is purely motor.
-
Superficial radial nerve is purely sensory.
-
Understanding the course is essential in trauma, fracture fixation, and surgical approaches around the arm and elbow.

Leave a Reply