Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Posterior Labral Tear & Posterior Shoulder Instability
Introduction
Posterior labral tears are injuries involving the:
- Posterior glenoid labrum
and are commonly associated with:
- Posterior shoulder instability
Patients may present with:
- Posterior subluxation
- Painful instability
- Rarely, frank posterior dislocation
Posterior instability is often subtle and frequently missed because symptoms are less dramatic than anterior instability.
Relevant Anatomy
Glenoid Labrum
The glenoid labrum is a fibrocartilaginous structure that:
- Deepens the glenoid socket
- Improves shoulder stability
The posterior labrum helps resist:
- Posterior translation of the humeral head
Important Terminology
Reverse Bankart Lesion
A reverse Bankart lesion refers to:
- Detachment of the posterior labrum from the posterior glenoid rim
Kim Lesion
A Kim lesion is:
- An incomplete concealed avulsion of the posteroinferior labrum
This lesion may appear normal unless specifically probed during arthroscopy.
Pathoanatomy and Risk Factors
Mechanism of Injury
Posterior labral injuries commonly occur due to:
- Axial loading of an adducted, internally rotated arm
Glenoid Retroversion
Increased glenoid retroversion significantly increases the risk of:
- Posterior shoulder instability
Common Injury Mechanisms
Traumatic Causes
A direct anterior blow to the shoulder may create:
- Posteriorly directed force on the humeral head
leading to posterior instability.
Repetitive Microtrauma
Repetitive loading is common in athletes performing:
- Pushing activities
- Weightlifting
- Contact sports
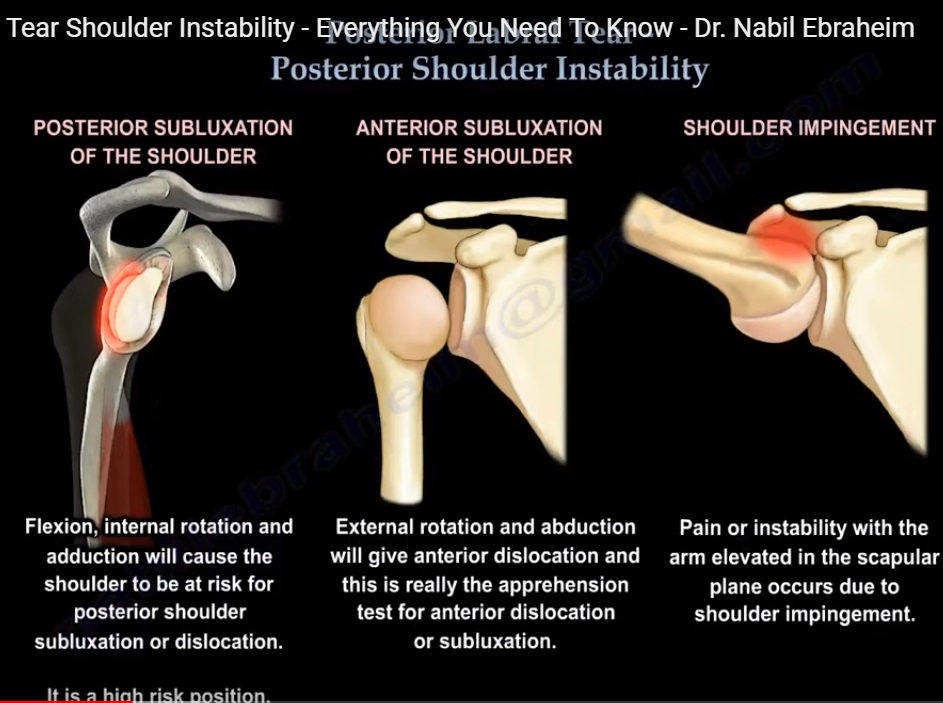
High-Risk Positions
Posterior Instability Position
Posterior instability commonly occurs in:
- Flexion
- Adduction
- Internal rotation
Anterior Instability Position
For comparison, anterior instability classically occurs in:
- Abduction
- External rotation
At-Risk Populations
Posterior instability is more common in:
- Contact athletes
- Football linemen
- Weightlifters
- Bench press athletes
- Overhead athletes
Clinical Presentation
Symptoms
Symptoms are often:
- Vague
- Subtle
- Pain-dominant rather than instability-dominant
Patients may describe:
- Shoulder slipping
- Weakness during pushing
- Pain with bench press
- Pain while blocking or throwing
True posterior dislocation requiring reduction is relatively uncommon.
Physical Examination
General Findings
Most patients demonstrate:
- Near-normal range of motion
- Normal rotator cuff strength
- Minimal muscle atrophy
Commonly Negative Tests
The following are often negative:
- Anterior apprehension test
- Sulcus sign
unless multidirectional instability is present.
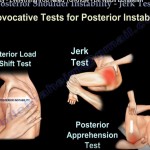
Special Tests
Jerk Test
Technique
- Arm positioned in 90° abduction and internal rotation
- Axial load applied
- Shoulder horizontally adducted
Positive Test
A positive test produces:
- Sudden jerk or clunk
- Posterior subluxation
- Pain
Kim Test
Technique
- Arm positioned in 90° abduction
- Axial load applied
- Upward and posterior force added
Positive Test
A positive Kim test causes:
- Sudden posterior shoulder pain
- Sometimes an associated click
This test is particularly sensitive for:
- Posteroinferior labral lesions
Diagnostic Accuracy
The combination of:
- Jerk test
- Kim test
provides approximately:
- 97% sensitivity
for posterior labral pathology.
Imaging
Plain Radiographs
X-rays may demonstrate:
- Posterior humeral head subluxation
- Glenoid retroversion
- Posterior glenoid erosion
MRI
MRI is the preferred initial imaging modality because it identifies:
- Posterior labral tears
- Capsular injury
- Associated soft tissue pathology
MR Arthrogram
MR arthrography improves sensitivity for:
- Labral pathology
- Capsular lesions
Important Imaging Pearl
Labral abnormalities may be present in asymptomatic athletes.
MRI findings must always be:
- Correlated clinically
Associated Lesions
Reverse Hill-Sachs Lesion
This refers to:
- Impaction fracture of the anteromedial humeral head
associated with posterior dislocation.
Paralabral Cyst
Posterior labral tears may be associated with:
- Paralabral ganglion cysts
These cysts may compress the:
- Suprascapular nerve
leading to:
- Infraspinatus weakness
- Reduced external rotation strength
Management
Non-Operative Treatment
Conservative management is first-line treatment.
Physiotherapy
Rehabilitation focuses on strengthening:
- Rotator cuff muscles
- Scapular stabilizers
Activity modification is also important.
Surgical Management
Indications
Surgery is indicated for:
- Failed conservative treatment
- Persistent symptomatic instability
Preferred Procedure
The preferred treatment is:
- Arthroscopic posterior labral repair
Open procedures are rarely required.
Postoperative Rehabilitation
Postoperative care typically includes:
- Initial immobilization
- Gradual physiotherapy progression
Patients should avoid:
- Passive adduction in a flexed position
to protect the repair.
Special Surgical Situations
Reverse Hill-Sachs Lesion
May require:
- McLaughlin procedure
- Lesser tuberosity transfer
- Subscapularis tendon transfer
Paralabral Cyst
Treatment may involve:
- Cyst decompression
- Labral repair
Complications
Nerve Injury
The posterior branch of the:
- Axillary nerve
lies very close to the inferior capsule and may be at risk during surgery.
The nerve supplies:
- Teres minor
- Lateral shoulder sensation
Over-Tightening
Excessive capsular tightening may result in:
- Shoulder stiffness
- Iatrogenic anterior instability
Differential Diagnosis
Conditions that may mimic posterior instability include:
- Rotator Cuff Tear
- Internal impingement
- SLAP lesions
- Multidirectional instability
- Cervical radiculopathy
Key Clinical Pearls
- Posterior instability is subtle and commonly missed.
- Push-related shoulder pain should raise suspicion.
- Weightlifters and contact athletes are high-risk groups.
- Jerk and Kim tests are highly valuable clinically.
- MRI findings must always correlate with symptoms.
- Paralabral cysts may cause suprascapular nerve compression.
- Arthroscopic posterior labral repair is the preferred surgical treatment.
Final Take-Home Message
Posterior labral tears and posterior shoulder instability are important but frequently underdiagnosed causes of shoulder pain in athletes and active individuals.
Patients commonly present with:
- Pain during pushing activities
- Sensation of instability
- Subtle mechanical symptoms
Careful clinical examination using:
- Jerk test
- Kim test
combined with appropriate imaging is essential for diagnosis.
Most patients improve with rehabilitation, while persistent symptomatic instability may require arthroscopic posterior labral repair.
Leave a Reply