POSTEROLATERAL CORNER (PLC) INJURIES
INTRODUCTION
-
Injuries to the posterolateral corner are functionally disabling and frequently challenging to diagnose.
-
Due to the complex anatomy and subtle clinical presentation, PLC injuries have historically been under-recognized.
-
Isolated PLC injuries are uncommon (?1.6%) and most often occur in combination with cruciate ligament injuries, particularly ACL or PCL tears (43–80%).
-
A high association exists with tibial plateau fractures (up to 68%).
-
Failure to identify and treat a PLC injury is a well-known cause of cruciate ligament reconstruction failure.
FUNCTION
-
The popliteus tendon functions synergistically with the PCL to control external tibial rotation, varus alignment, and posterior tibial translation.
-
The popliteus–popliteofibular ligament complex provides maximal restraint to external rotation when the knee is flexed.
-
The lateral collateral ligament (LCL) is the primary restraint to varus stress, contributing approximately:
-
55% at 5° of knee flexion
-
69% at 25° of knee flexion
-
ETIOPATHOGENESIS
-
Common causes include:
-
Sports-related trauma (?40%)
-
Motor vehicle accidents
-
Falls from height
-
Mechanisms of injury:
-
Direct blow to the anteromedial aspect of the knee
-
Hyperextension injuries
-
Varus loading forces
-
Non-contact mechanisms involving hyperextension, varus stress, or excessive external tibial rotation
Role of PLC:
-
The PLC resists lateral joint opening and prevents varus thrust during gait.
CLINICAL FEATURES
Acute phase:
-
Posterolateral knee pain
-
Swelling
-
Anteromedial joint line tenderness
Chronic phase:
-
Subjective instability
-
Varus thrust gait
-
Difficulty with running and cutting activities
-
Episodes of giving way, especially during stair descent or pivoting movements
EXAMINATION FINDINGS
Acute signs:
-
Knee swelling
-
Ecchymosis and abrasions
-
Antalgic gait
Chronic signs:
-
Varus malalignment
-
Asymmetric knee hyperextension
-
A thorough assessment of peroneal nerve function is essential due to the risk of associated nerve and vascular injury.
SPECIAL TESTS
-
External rotation recurvatum test
-
Posterolateral drawer test – suggests injury to the popliteus tendon or popliteofibular ligament
-
Varus stress test
-
Dial test
-
Increased external rotation at 30° ? isolated PLC injury
-
Increased rotation at 30° and 90° ? combined PLC and PCL injury
-
-
Reverse pivot shift test – demonstrates posterior tibial subluxation with sudden reduction
CLASSIFICATION
Grading of PLC Injuries:
-
Grade I: Mild instability (0–5 mm or 0–5°)
-
Grade II: Moderate instability (6–10 mm or 6–10°)
-
Grade III: Severe instability (>10 mm or >10°)
INVESTIGATIONS
Radiographs
-
Segond fracture (lateral or medial)
-
Arcuate sign (fibular styloid avulsion) – pathognomonic for PLC injury
-
Gerdy’s tubercle avulsion
-
Lateral joint space widening
MRI
-
Grade I: Periligamentous T2 hyperintensity
-
Grade II: Increased signal within an intact ligament
-
Grade III: Complete ligament disruption with surrounding edema
TREATMENT
Non-operative Management
Indications: Grade I injuries or minimal functional impairment
-
Hinged knee brace in extension for 6 weeks
-
Gradual progression of range of motion and weight bearing
-
Strengthening exercises
-
Return to activity at approximately 3–4 months
OPERATIVE MANAGEMENT
Indications:
-
Avulsion injuries
-
Multiligament knee injuries
-
Grade III PLC injuries
-
Acute repair within 3–4 weeks is preferred.
-
Fixation options include sutures, suture anchors, or bio-screws.
Surgical options include:
-
PLC repair
-
Hybrid PLC repair and reconstruction
-
PLC reconstruction with or without ACL reconstruction, PCL reconstruction, and/or high tibial osteotomy (HTO)
PLC REPAIR
Indications:
-
Isolated, acute Grade II PLC avulsion injuries
Limitations:
-
Midsubstance repairs are associated with failure rates of approximately 40%
Techniques:
-
Repair of the LCL, popliteus tendon, and/or popliteofibular ligament when anatomical reduction is achievable
-
Reconstruction is recommended when reduction is not possible or tissue quality is poor
-
Augmentation with a free graft may be used when repair is tenuous
-
Fibular head avulsion fractures can be fixed using screws or suture anchors
HYBRID PLC RECONSTRUCTION AND REPAIR
Indications:
-
Grade III midsubstance injuries
-
Irreparable avulsion injuries
-
Poor tissue quality
Techniques:
-
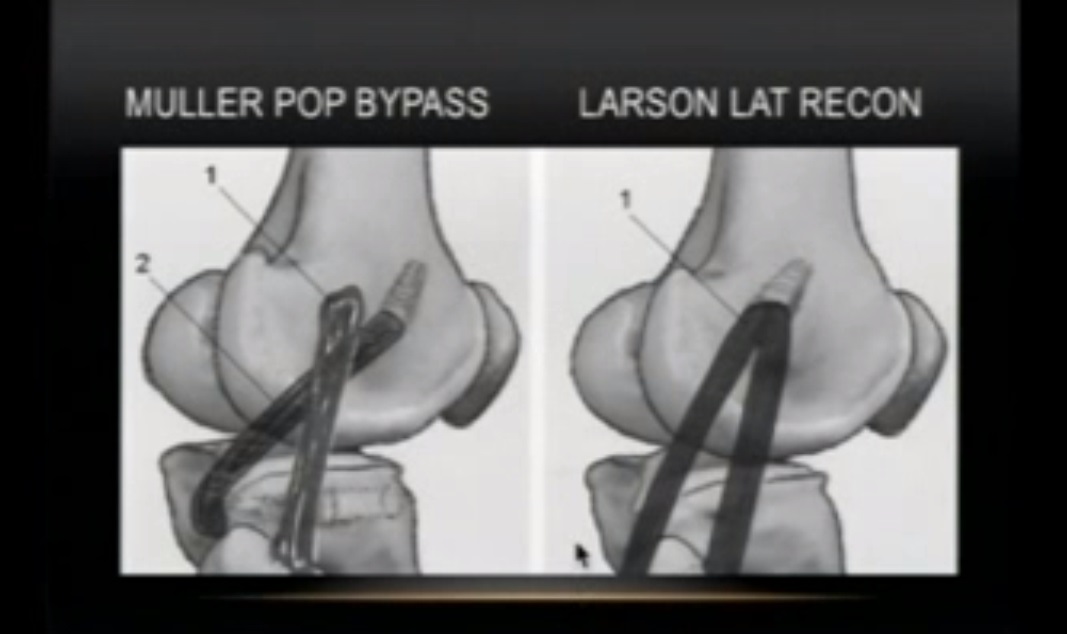
Larson (fibular-based) reconstruction
-
Trans-tibial double-bundle reconstruction
-
LaPrade anatomic reconstruction
REHABILITATION
-
Hinged knee brace with non-weight bearing for 6 weeks
Range of motion:
-
Either immediate passive ROM (0–90°), or
-
Immobilization for 2 weeks followed by gradual motion
-
At 6 weeks: initiate weight bearing and closed-chain strengthening
-
Return to sports and high-level activities at approximately 6–9 months
OUTCOMES
-
Operative management yields superior outcomes compared to non-operative treatment
-
Reconstruction demonstrates lower failure rates than repair
-
Early intervention is associated with improved functional results
-
Anatomic reconstruction restores rotational stability, although complete restoration of varus stability may not always be achieved
PLC RECONSTRUCTION ± ACL / PCL RECONSTRUCTION ± HTO
Indications:
-
Acute or chronic combined ligament injuries
Principles:
-
PLC reconstruction should be performed prior to or concurrently with ACL or PCL reconstruction to prevent early graft failure
-
Valgus high tibial osteotomy is indicated in patients with varus mechanical alignment
-
Failure to correct coronal plane malalignment significantly compromises reconstruction outcomes
Reconstruction techniques:
-
Non-anatomic: Biceps tenodesis, iliotibial band sling, arcuate complex reconstruction
-
Anatomic (preferred): LaPrade-style anatomic reconstruction or fibular-based Larson technique
-
Key structures addressed include the LCL, popliteofibular ligament, and popliteus tendon
-
The Larson technique is technically simpler and effective but may risk over-constraint if graft tensioning is not balanced
COMPLICATIONS
-
Arthrofibrosis
-
Missed PLC injury
-
Failure to recognize PLC injury leading to ACL or PCL reconstruction failure
-
Peroneal nerve injury (15–29%)
Leave a Reply