Courtesy: Hitesh Shah, Paediatric Orthopaedic Surgeon, Manipal, India
Ponseti Method of Clubfoot Management
Introduction
-
Manipulation and casting provide superior, simpler, and faster outcomes compared to surgical intervention in the management of clubfoot.
-
The Ponseti method is:
-
Easy to learn
-
Cost-effective
-
Minimally invasive
-
Highly effective when performed correctly
-
-
It is currently considered the gold standard for the treatment of idiopathic clubfoot.
Topics Covered
-
Objectives of treatment
-
Types of clubfoot
-
Deformities in clubfoot
-
Aims of treatment
-
Ponseti manipulation technique
-
Atypical clubfoot
-
Common errors
-
Limitations of manipulation
Types of Clubfoot
-
Primary idiopathic clubfoot
-
Secondary clubfoot
-
Neurogenic causes such as spina bifida
-
Multiple congenital contractures
-
Associated syndromes including:
-
Larsen syndrome
-
Diastrophic dysplasia
-
Möbius syndrome
-
-
Deformities in Clubfoot
Hindfoot Equinus
-
The heel is elevated and does not touch the ground.
-
On lateral view, the angle between the tibial axis and foot axis is greater than 90 degrees.
-
Normally, the plantar foot makes a right angle with the table surface.
Hindfoot Varus
-
The heel is deviated medially.
-
In a normal foot, the heel bisects the calcaneum.
-
In clubfoot, medial deviation occurs due to subtalar joint deformity.
-
Hindfoot varus results from adduction, inversion, and plantar flexion at the subtalar joint.
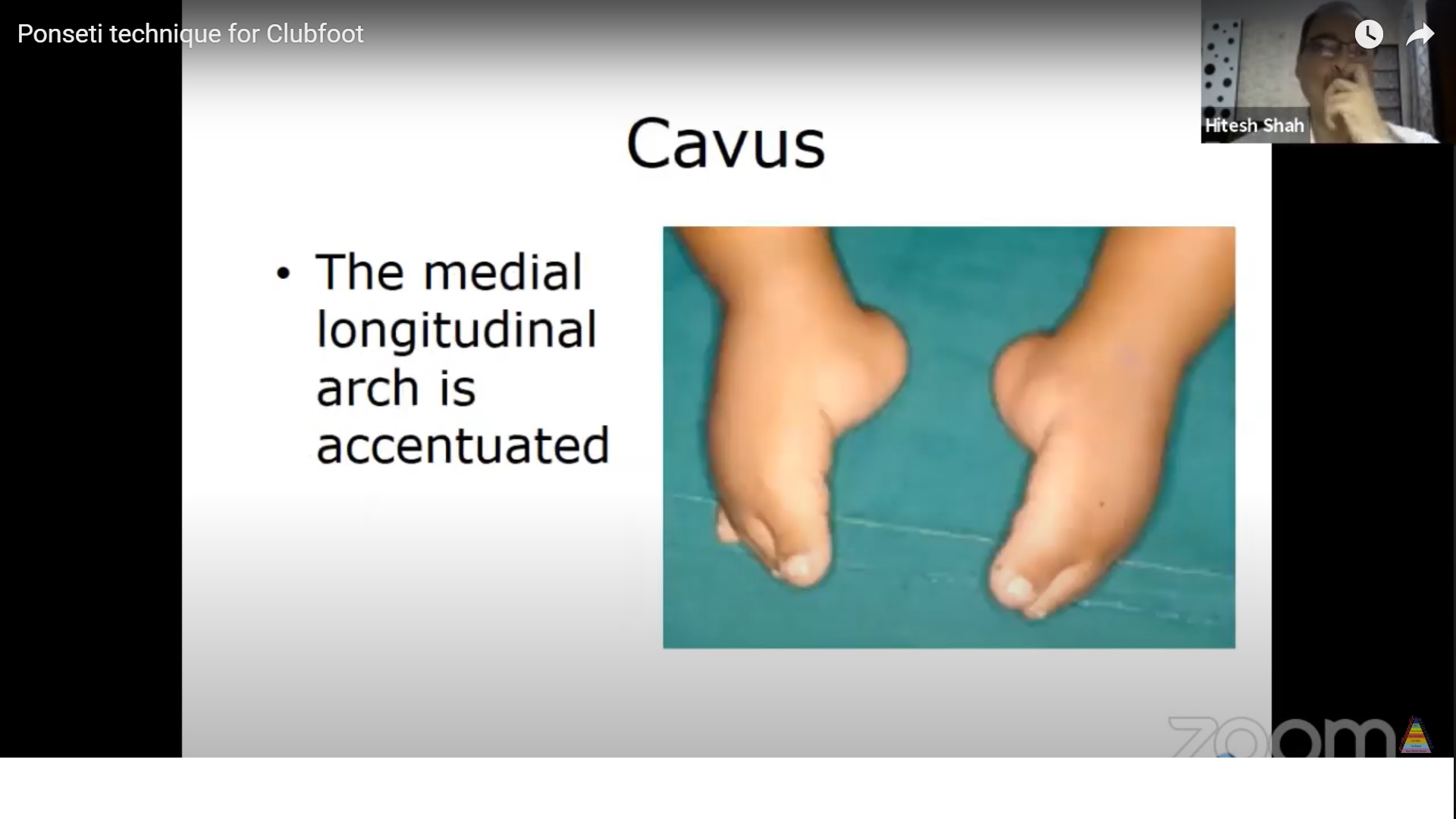
Cavus
-
The medial longitudinal arch is accentuated.
-
The first ray is plantar flexed.
-
The lateral border of the foot contacts the ground.
Forefoot Adduction
-
The medial and lateral borders of the foot are curved.
-
The foot cannot be aligned in a straight axis.
Findings in Dissected Specimens
Equinus
-
Severe plantar flexion at the tibiotalar and talocalcaneal joints.
Adduction
-
Medial inclination of the talar neck.
-
Medial displacement of the navicular and cuboid.
-
Calcaneus is adducted.
-
Forefoot is adducted relative to the hindfoot.
Varus
-
Calcaneus is adducted, plantar flexed, and inverted.
Cavus
-
Plantar flexion of the first metatarsal.
Pirani Scoring System
Hindfoot Score
Posterior Crease
-
0: Absent
-
0.5: Faint
-
1: Deep
Empty Heel
-
0: Calcaneum palpable
-
1: Calcaneum not palpable
Rigid Equinus
-
0: Passive dorsiflexion beyond neutral
-
0.5: Passive dorsiflexion to neutral
-
1: No dorsiflexion, fixed at 90 degrees
Midfoot Score
Medial Crease
-
0: Absent
-
0.5: Faint
-
1: Deep
Lateral Head of Talus
-
0: Not palpable
-
0.5: Palpable but not prominent
-
1: Prominent and palpable
Curved Lateral Border
-
0: Forefoot touches straight line
-
0.5: Forefoot partially touches straight line
-
1: Forefoot does not touch straight line
Interpretation of Pirani Score
-
Score ranges from 0 to 6
-
0 indicates complete correction
-
6 indicates severe deformity
-
Forefoot deformity should be corrected first
-
Midfoot score should be 0 or 0.5 before addressing hindfoot equinus
Goals of Treatment
-
Functional foot
-
Pain-free foot
-
Plantigrade foot
-
Mobile foot
Ponseti Technique
-
A specific method of serial manipulation and casting
-
Uses the head of the talus as a fulcrum
-
Followed by tendo-Achilles tenotomy in most cases
Goals of Plaster Manipulation
-
Begin treatment as early as possible, ideally within 1 week of birth
-
Change casts every 5 to 7 days
-
Endpoint is complete correction of all deformities
Order of Deformity Correction
-
Cavus
-
Adduction
-
Varus
-
Equinus
Rationale
-
Attempting to correct equinus first can lead to rocker-bottom deformity
-
Following the correct sequence prevents secondary deformities
Stages of Correction
Step 1: Cavus Correction
-
Achieved by elevating the first metatarsal
-
First and fifth metatarsals are brought into the same plane
-
This corrects forefoot pronation and is termed supination of the forefoot
-
Thumb is placed over the head of the talus to provide counter-pressure
Step 2: Correction of Adduction and Varus
-
The head of the talus is used as a fulcrum
-
Forefoot is gradually abducted while maintaining supination
-
Navicular shifts laterally
-
Gradual abduction up to 70 degrees is required
-
Hindfoot varus corrects automatically with forefoot abduction
-
Pronation of the foot should never be performed
Casting Technique
-
Manipulation is maintained for 30 to 40 seconds
-
Casting is applied immediately after manipulation
-
Above-knee cast is applied with:
-
Knee flexed to 90 degrees in children under 1 year
-
Knee flexed to 40 to 60 degrees in older children
-
-
All casts are applied without anesthesia or sedation
Step 3: Correction of Hindfoot Equinus
-
Most children require tendo-Achilles tenotomy
-
Forceful manipulation of equinus should be avoided
-
Incorrect manipulation may cause rocker-bottom deformity
Tendo-Achilles Tenotomy
Indications
-
Midfoot score less than 1
-
Hindfoot score greater than 1
Goals
-
Achieve at least 15 degrees of ankle dorsiflexion
Technique
-
Performed under local or general anesthesia
-
Tendon is completely transected
-
Dorsiflexion should occur at the tibiotalar joint, not the midtarsal joint
-
Performed using a needle or blade
-
Care is required due to medial neurovascular structures
Post-Procedure Care
-
Foot is maintained for 3 weeks
-
Position:
-
15 degrees dorsiflexion
-
70 degrees abduction
-
Foot Abduction Orthosis
Usage
-
Worn 23 hours per day until walking age, minimum 3 months
-
Daytime wear continued until 4 years of age
Measurements
-
Bar length equals the distance between the child’s shoulders
Care
-
Ensure heel is seated properly in the shoe
-
Ankle strap must be secured firmly
-
Hindfoot equinus correction must be maintained
Discontinuation of Orthosis
-
When the child can actively abduct and invert the foot
-
Some children may develop dynamic supination due to tibialis anterior overactivity
-
These cases may require tibialis anterior tendon transfer
Number of Casts Required
-
Depends on:
-
Age of the patient
-
Severity of deformity
-
Degree of soft tissue tightness
-
Atypical Clubfoot
-
Short first metatarsal
-
Dorsiflexed first metatarsophalangeal joint
-
Deep plantar creases
-
All metatarsals plantar flexed
Treatment
-
Apply targeted pressure to correct plantar flexed metatarsals
Limitations of Ponseti Method
-
Approximately 95 percent achieve complete correction
-
Limitations occur when:
-
Navicular is fixed with false correction
-
Subtalar joint is fixed, commonly in secondary clubfoot
-
Common Errors
-
Failure to correct cavus by elevating first metatarsal
-
Pronation or eversion of the foot
-
Premature attempt to correct equinus
Follow-Up
-
Long-term follow-up is mandatory for all children
-
Relapses can occur if bracing protocol is not followed
Age Limit for Ponseti Method
-
Initially used up to 2 or 3 years of age
-
Currently, no upper age limit is defined
Key Principles of Ponseti Method
-
Correct sequence of deformity correction is essential
-
Elevation of first metatarsal is critical
-
Counter-pressure must be applied on the lateral aspect of the talar head
-
Heel varus corrects with abduction
-
Tendo-Achilles tenotomy is required in most cases

a very good lecture and very well explained each aspect of this deformity, wish that there is one lecture on vertical talus, rocker bottom foot as well