Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
- Also known as Ledderhose’s disease.
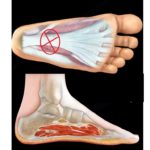
- It is a benign tumour of the plantar fascia of the foot.
- It consists of myofibroblasts and dense fibrous proliferation infiltrating the adipose tissue. It is most often found in the central and medial portion of the plantar fascia.
- The firm nodule is located on the medial border of the sole of the foot.
- The nodule is close to the skin and gradually increases in size.
- It is painful with wearing shoes.
- This condition is bilateral in about 25% of patients. Early lesions are more cellular.
- Biopsy could be misdiagnosed as fibrosarcoma.
- Older lesions have less cells and more collagen.
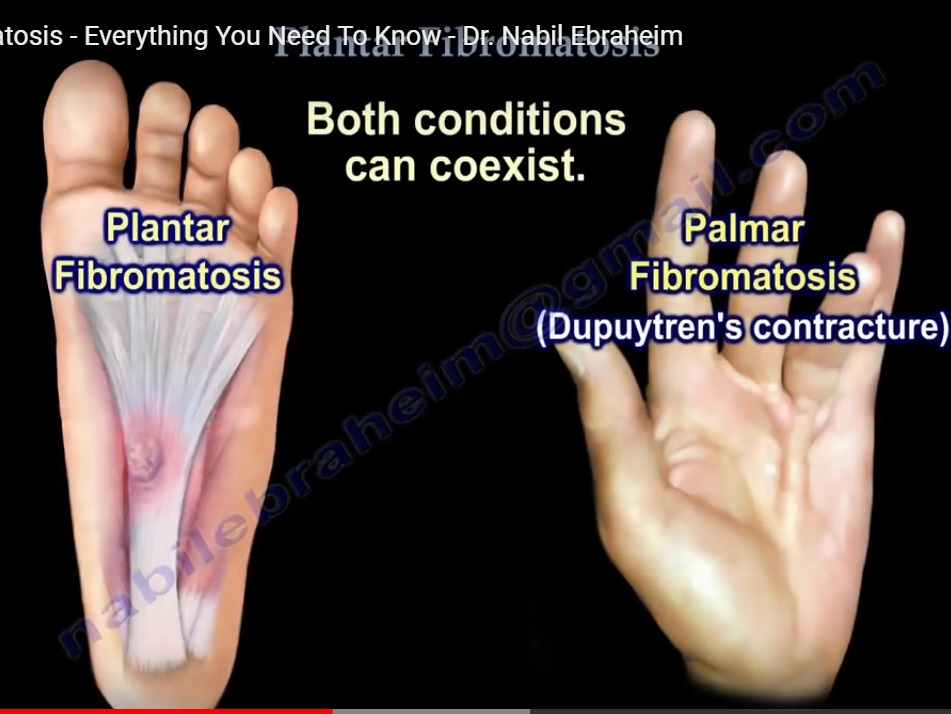
Plantar fibromatosis of the foot is different from palmar fibromatosis of the hand which cause dupuytrens contracture.
Plantar fibromatosis and palmar fibromatosis can co-exist. However there is no contracture with plantar fibromatosis.
- Plantar fibromatosis can result from fibroblast proliferation with infiltrative growth that is easily recognised clinically.
- If the mass is suspicious, then an MRI or Ultrasound may help with the diagnosis.
- MRI and Ultrasound will also show the extent of the lesion. Ultrasound will show diffuse,discrete fusiform thickening of the plantar fascia.
- Lesion can be multiple and bilateral.
- The superficial fibres are more affected. It’s often difficult to differentiate between a chronic partial tear and a nodule.
- There is no relationship between the symptoms and the ultrasound appearance.
- The ultrasound appearance is usually characteristic.
The etiology of plantar fibromatosis is multifactorial- trauma,familial,diabetes,
Plantar fibromatosis occur in adults and is rare before the age of 30. It occurs more in males than females.
Treatment :
- Non-operative: accommodative footwear and inserts.
- If the lesion is excised it will lead to a high rate of recurrence.
- The best treatment is wide resection of the fascia( lower recurrence rate) especially with large modules that cause severe pain or nerve compression.
- Do not operate on painful nodules at the bottom of the foot as they may come back worse than before.
- It is important to study the nature of painful modules before operating on them. Make sure that the proper surgery is chosen for it.
- A local lesion will cause recurrence of the lesion due to the infiltrative nature ( the lesion is not encapsulated).
- Post- operative radiation therapy for aggressive fibromatosis was found to improve local control of the lesion. If the mass appears suspicious,a biopsy may be needed to rule out soft tissue sarcoma, such as synovial cell sarcoma
It is rare to find any medical professional who manages the whole patient with Dupuytrens and plantar fibromatosis. Orthopedists vs Podiatrists seem unable to identify triggers for intermittent fibroplastic growth. Yet these conditions are not constantly evolving. A patient can tell when their hands are in a proliferation phase and when the conditions are temporarily dormant. Is there work being done or information to be had to identify what triggers exacerbation? Interrupting the process would save functionality or at least delay the deterioration. Thanks