Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Sequence of Examination
-
Gait
-
Inspection
-
Palpation
-
Movements
-
Measurements
-
Special tests
-
Neurological examination
1. Gait Assessment
Observe the patient walking normally and while turning.
-
Shuffling gait
-
Slap foot gait
-
Broad-based or halting gait
-
Antalgic gait
-
Trendelenburg gait
-
High-stepping gait
-
Hemiplegic or circumduction gait
2. Inspection
Inspection should be performed from the front, side, and back with the patient standing upright and adequately exposed.
Inspection from the Front
-
Normally, the head and neck are aligned with the chest and lower spine.
-
In torticollis:
-
The neck is tilted to one side.
-
The chin is rotated to the opposite side.
-
-
Facial tilt may be seen in acquired torticollis due to:
-
Tonsillar infection
-
Vertebral body infection
-
Klippel–Feil syndrome
-
-
Compare both sternocleidomastoid muscles for:
-
Symmetry
-
Swelling (sternomastoid tumor)
-
Tightness or unilateral shortening, suggestive of congenital muscular torticollis
-
-
Observe the supraclavicular fossae:
-
Normally hollow
-
Fullness may indicate abscess, Pancoast tumor, or rarely a complete bony cervical rib
-
Inspection from the Side
-
Ask the patient to stand erect.
-
Assess normal spinal curvatures:
-
Cervical lordosis
-
Thoracic kyphosis
-
Lumbar lordosis
-
Abnormal Findings
-
Loss of cervical lordosis:
-
Seen in ankylosing spondylitis
-
-
Knuckle deformity:
-
Collapse of a single vertebra
-
-
Angular deformity:
-
Collapse of 2 to 3 vertebrae
-
-
Round back deformity:
-
Collapse of 4 or more vertebrae
-
-
Exaggerated lumbar lordosis (hyperlordosis), usually compensatory:
-
Developmental dysplasia of the hip
-
Flexion deformity of the hip
-
Spondylolisthesis
-
-
Loss of lumbar lordosis:
-
Ankylosing spondylitis
-
Intervertebral disc prolapse due to muscle spasm
-
Spinal infections
-
Vertebral compression fracture
-
Degenerative disc disease
-
Inspection from the Back
-
Both shoulders and iliac crests should be at the same level.
-
Head, neck, spine, and natal cleft should lie in a straight vertical line.
-
Look for:
-
Scoliosis
-
Step-off deformity
-
Surgical scars
-
Sinuses
-
Swelling
-
3. Palpation
Palpate gently and systematically.
-
Local rise of temperature
-
Spinal tenderness
-
Alignment of spinous processes
-
Step-off between adjacent spinous processes
-
Paraspinal muscle spasm
-
Any swelling or scars
4. Movements
Assess active and passive movements and note pain, restriction, or spasm.
Cervical Spine Movements
-
Flexion (sagittal plane): 0 to 80 degrees
-
Extension (sagittal plane): 0 to 50 degrees
-
Lateral bending (coronal plane): 0 to 45 degrees
-
Rotation (axial plane): 0 to 80 degrees
Lumbar Spine Movements
-
Flexion
-
Extension
-
Lateral bending
-
Rotation
5. Measurements
-
Chest expansion
-
Modified Schober test
-
Wall–occiput distance
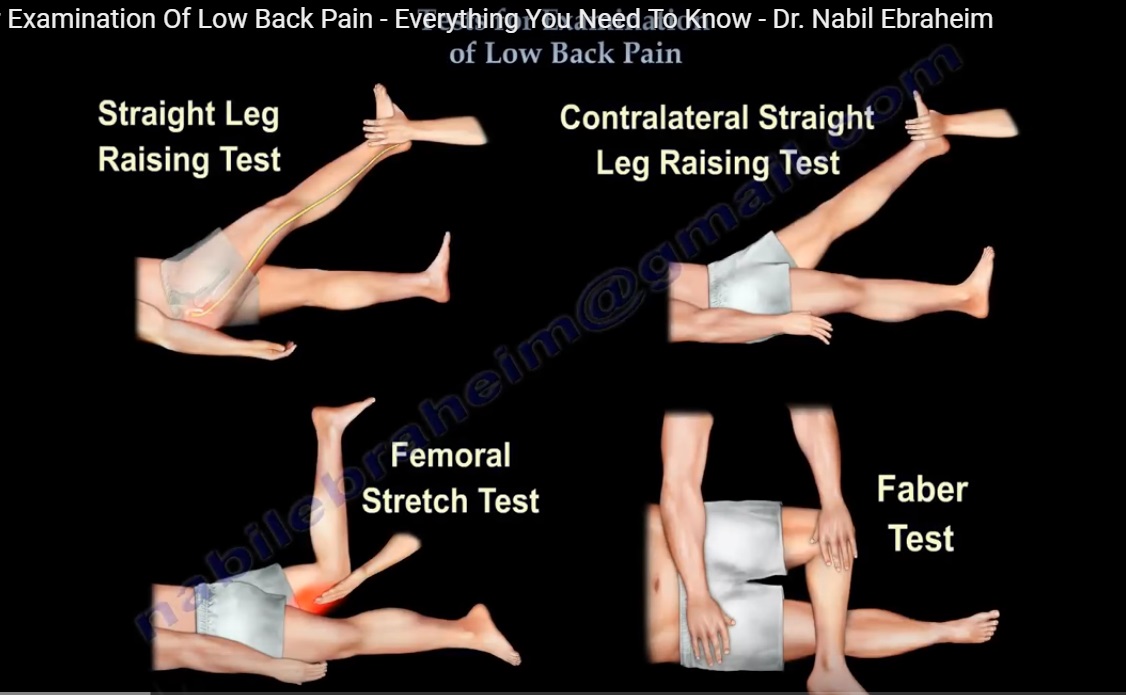
6. Special Tests
Lumbar Spine and Nerve Root Tests
-
Straight leg raising test (Lasegue test)
-
Bragard test
-
Bowstring sign
-
Femoral nerve stretch test
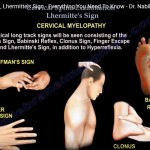
Cervical Spine Tests
-
Lhermitte maneuver
-
Axial compression test
-
Spurling test
-
Cervical distraction test
Other Tests
-
Beevor sign
-
Figure-of-four test
-
Adson test
-
Roos test
-
Romberg test
7. Neurological Examination
-
Motor examination of upper and lower limbs
-
Sensory examination
-
Deep tendon reflexes
-
Pathological reflexes when indicated
-
Rectal examination when required to assess:
-
Sacral nerve function
-
Cauda equina involvement
-
Summary
-
Spine examination must be systematic and sequential.
-
Inspection and gait often provide early diagnostic clues.
-
Movements, measurements, and special tests help localize pathology.
-
A complete neurological examination is essential in all patients with spinal complaints.

Leave a Reply