Courtesy: Amr Abdelgawad, Maimonaides Medical Centre, Brooklyn, New York, USA
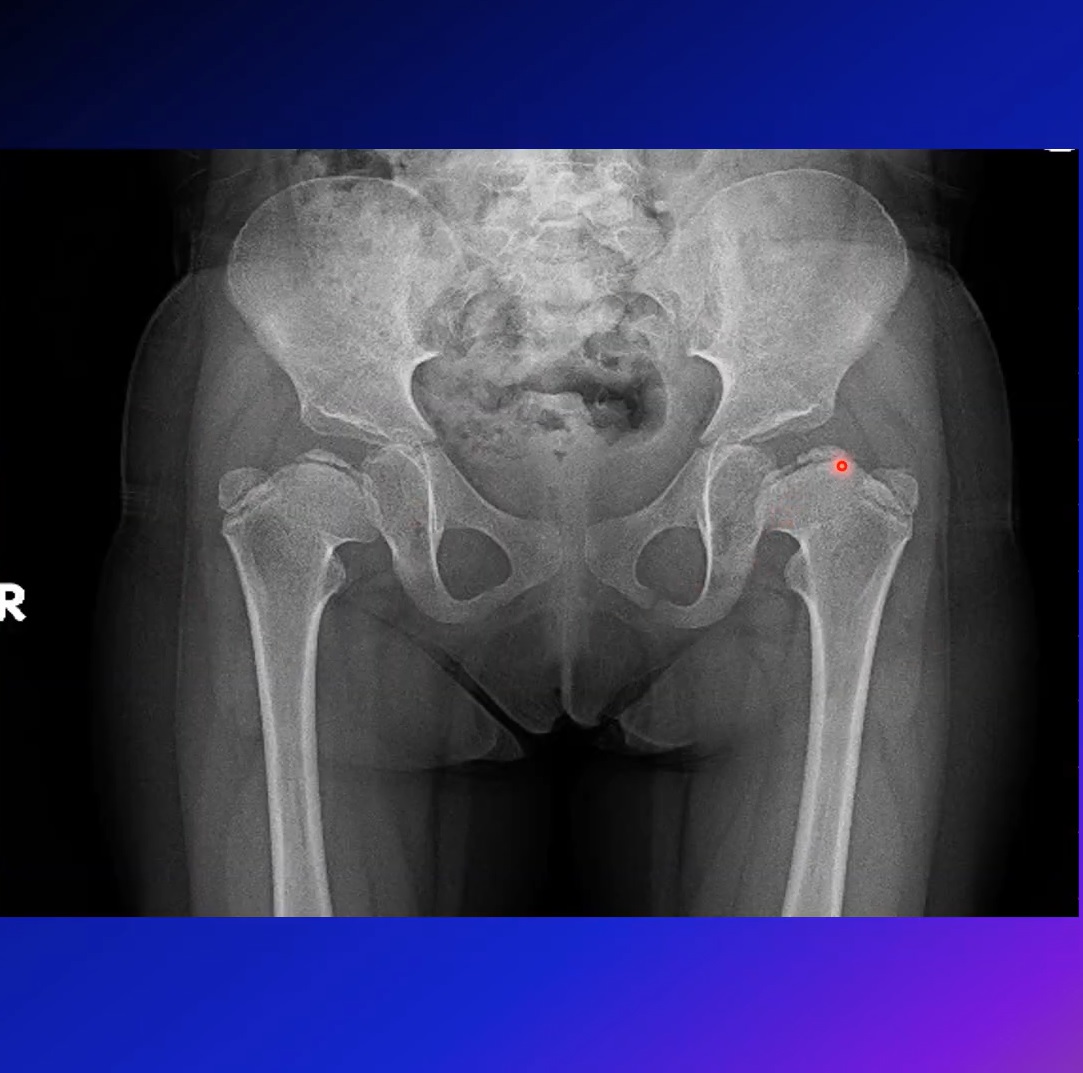
LEGG-CALVÉ-PERTHES DISEASE
Introduction
• Idiopathic avascular necrosis of the proximal femoral epiphysis
• Approx 1 in 1000 children
• m/c between 4 and 8 years of age
• Increased incidence in Northern Europe
• Caucasians and Chinese are significantly more affected
• Boys : girls is 5:1
• 10% are bilateral and is common in girls
• In bilateral both hips may be in different stages of the disease process
History
LCPD described in 1910 by
• Arthur Legg of the United States,
• Jacques Calvé of France,
• Georg Perthes of Germany,
• Henning Waldenström of Sweden
• Legg described the prominent characteristics of the disorder
• Calvé noted that affected individuals had minimal atrophy of the leg and no palpable hip swelling
• Perthes observed the disorder as “a self- limiting, noninflammatory condition, affecting the capital femoral epiphysis with stages
• Waldenström reported the radiographic changes associated with the disorder in 1909
Risk factors
• Low birth weight,
• Exposure to secondhand cigarette smoke,
• Short body length at birth,
• Family history,
• Low socioeconomic status
• Attention deficit hyperactivity disorder type 1(ADHD-1)
Asso. with congenital abnormalities like
• Genitourinary malformations, undescended testes, inguinal hernia, Down’s syndrome and some coagulopathies
Pathology
• Disruption of blood supply to the femoral head, is one of the key pathogenic event
• Microtrauma to retinacular vessels
• Increased synovial pressure
• eg: Transient synovitis
• Venous HTN 2° to thrombotic occlusion
• Single ischemic episode or multiple ischemic events
Pathogenesis & pathology
• Repeated bouts of ischaemia & infarction of femoral head? pathologic fractures
• Retinacular vessels susceptible to stretching & pressure from effusion
• Increased pressure cause venous stasis
• Increase in intraosseous pressure
• Ischaemia & infarction leading to necrosis
Pathogenesis of femoral head deformity
• Pathogenesis of the femoral head deformity following ischemic necrosis is complex
• Multiple factors contribute to the development of the deformity
1. Mechanical properties of the articular cartilage and the bone are decreased
• Necrosis of the deep layer of the articular cartilage
• Inability of the necrotic bone to repair microdamage
• Increase in the calcium content of the calcified cartilage and the subchondral bone making it brittle
• When mechanical loading > strength of bone = subchondral fractures & collapse
2. Pathological repair process
• Predominance of osteoclastic resorption
• Delayed bone formation
• replacement of the necrotic bone by a fibrovascular granulation tissue
3. Growth arrest of the spherical growth plate• Restoration of growth in asymmetrical manner
Clinical features
• Typically a boy of 4-8 years who has high physical activity
• C/O pain & limping
• Maybe painless limp
• Pain may radiate to knee
• Aggravated by strenuous activity & relieved by rest
• Continuous for weeks or intermittent
• Urogenital anomaly in 4%
• Leg length discrepancy
• Mild muscle wasting
ROM
• Early: joint irritable, decreased ROM & painful in extremes
• Later: Movements full except Abduction & IR
• Maybe flexion / adduction contracture
• Gait: Antalgic or Trendelenburg / Abductor gait
• Trendelenburg test: +ve
Diagnosis
• Based on clinical features & Radiology
Investigations:
• Routine blood investigation
X-ray
• Initially normal
• Subtle changes: widening of joint space, asymmetry of ossification centres
• Necrotic phase: Increased density of ossific nucleus
• Fragmentation phase: Alternating patches of density & lucency
• Crescent sign (best seen on lateral view)
• Re-ossification phase: Increased epiphyseal density
MRI:
• Evidence of marrow necrosis
• Irregularity of the femoral head,
• Loss of the signal on the affected side
Bone scan:
• Reduced uptake early in the disease
Ultrasound
• Joint effusion
Arthrography:
• To see congruity, head deformity
Classification
• Waldenstorm classification – Stages of disease
• Catterall classification – Degree of femoral head involvement
• Herring classification – Height of lateral pillar
• Modified Elizabethtown classification – Evolution of disease
• Salter-Thompson Classification – Extent of subchondral fracture
• Stulberg Criteria – Femoral head shape and Acetabular fit
Waldenstrom Classification
Stage 1: Initial phase
• All or part of nucleus dead. Maybe normal X-ray. Increased density of epiphysis
• Cartilage thickening, subtle lateral subluxation via increased medial cartilage growth (Waldenstram’s sign]
• Subcondral Fracture/collapse (Crescent sign)
• Duration: 6 months
Stage 2:Fragmentation phase
• Areas of lucency and sclerosis
• Central area separates from lateral & medial areas
• Maximal flattening/ collapse
• Duration: 8 months
Stage 3:Reossification phase
• New subchondral bone formation
• Flattening may improve
• Duration: 3-5 years
Stage 4: Residual phase
• No change in bone density
• Shape of head changes
• Final shape after skeletal maturity
• Acetabular remodelling
Catterall Classification
• Based on extent of head involvement and outcome
• Applied during fragmentation stage when the necrotic segment is demarcated from the viable portion
• At-risk signs that are associated with poor outcomes
• Gage sign (V-shaped radiolucency in the lateral portion of the epiphysis and/or adjacent metaphysis)
• Calcification lateral to the epiphysis
• Metaphyseal cyst
• Lateral subluxation of the femoral head
• Horizontal proximal femoral physis
• Group l : Normal height of epiphysis & 50% ht
• C: Severe collapse <50% ht
• Herring A: All do well without any treatment
• Herring B: Bone age 8: Surgery (Femoral/Salter) > Brace > No treatment
• Herring C: Bone age Brace > No treatment
• Herring C: Bone age >8: Poor outcome irrespective of treatment
Modified Elizabethtown classification
Stage Ia – Sclerosis of the epiphysis with no loss of height
Stage Ib – Sclerosis of the epiphysis with loss of height but no fragmentation
Stage IIa – Early fragmentation with just one or two vertical fissures in the epiphysis on the AP or frog leg lateral view
Stage IIb – Advanced fragmentation with no new bone lateral to the fragmented epiphysis
Stage IIIa – early “porotic” new bone formation at the periphery of the epiphysis covering less than a third of the epiphysis
Stage IIIb – New bone formation of “normal” texture and covers more than a third of the epiphysis.
Stage IV – Complete healing with no radiographically identifiable avascular bone.
Salter-Thompson Classification
• Group A: Subchondral # involving 50 % of head
• Applicable before fragmentation
Stulberg criteria for prognosis
• Radiographic appearance of hip at skeletal maturity
• Based on the femoral head shape and acetabular fit
• Gold standard for rating residual femoral head deformity and joint congruence
• Recent studies show poor interobserver and intra observer reliability
I – normal shaped femoral head and acetabulum
II – spherical femoral head, but with at least one type of deformation including coxa magna, shortened neck, or steep acetabulum
III – ovoid femoral head with congruently ovoid acetabulum and neck
IV – flat femoral head with congruently flat acetabulum and neck
V – flat femoral head with normal acetabulum and neck; incongruently incongruous.
Differential diagnosis
KNOWN CAUSES OF AVASCULAR NECROSIS
• Sickle cell disease
• Other hemoglobinopathies (e.g., thalassemia)
• Chronic myelogenous leukemia
• Steroid medication
• Sequela of traumatic hip dislocation
• Treatment of developmental dysplasia of the hip
• Septic arthritis?
SKELETAL DYSPLASIAS MIMICKING PERTHES
• Multiple epiphyseal dysplasia
• Spondyloepiphyseal dysplasia
• Mucopolysaccharidoses
• Hypothyroidism?
OTHER SYNDROMES
• Osteochondromatosis
• Metachondromatosis
• Schwartz-Jampel syndrome
• Trichorhinophalangeal syndrome
• Maroteaux-Lamy syndrome
• Martsolf syndrome
• Stickler syndrome
Management
Principles:
• Restore & maintain ROM
• Increases joint nutrition
• Prevents subluxation
• Allow abduction
• Satisfactory = 30° ABD
• Avoid treatment of patients who will do well without treatment
• Concept of containment
• Relief of symptoms
Objective: Preserve the sphericity of the femoral head
• Reduce the risk of stiffness and degenerative arthritis
• Preserving the emotional well-being of the child.
Determined by
• Age
• Extent of involvement
• Stage of disease
• Head at risk signs
Age
• Older the child the poorer the outcome
• Extremely poor outcome in adolescents
• Age 60% do not require surgery
• Observation, activity restriction, traction & physiotherapy
Indications:
• <6 years age
• Herring A
Bracing / Casting
• Petrie cast
• Atlanta Scottish Rite brace
• Bed rest with skin traction until the synovitis subsides (4 to 14 days)
• Children 2 to 3 years old can be observed and don’t need aggressive treatment.
• If significant loss of motion & lateral subluxation:
• Closed reduction + adductor tenotomy
• Petrie cast
• Satisfactory clinical results can be obtained at long-term follow-up despite an unsatisfactory radiographic appearance
Containment Surgery
• Timing of surgery: More important than the type of surgery
• Should be done before irreversible deformation of the femoral head occurs
Inominate osteotomy
Advantages:
• anterolateral coverage of the femoral head,
• lengthening of the extremity
• avoidance of a second operation for plate removal
Disadvantages:
• Inability to obtain proper containment
• Increased acetabular & joint pressure
• Increase leg length causing relative adduction
Varus derotational osteotomy
Advantages
• Seats the head deeply in acetabulum
• Removes vulnerable ant/lat portion from acetabular edge
• Decrease joint reaction forces
Disadvantages
• Excessive varus angulation (especially in an older child)
• Limb shortening, Trendelenburg gait
• Nonunion, Hardware removal
• Premature closure of the capital femoral physis may cause further varus deformity & trochanteric overgrowth
Arthrodiastasis
• Distraction of joint
• Widens joint space
• Unloading of joint
• Allows fibrous repair of cartilage defects
• Preserves congruency
• Articulated fixator allows 50° flexion
Complications
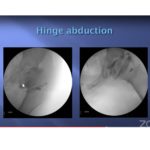
• Hinge Abduction
• Coxa breva
• Trochanteric overgrowth
• Coxa irregularis
• FAI
• Early OA
Management of Complications
Reconstructive surgeries and salvage procedures
• Valgus osteotomy
• Cheilectomy
• Shelf procedure
• Chiari osteotomy
• Trochanteric advancement
Valgus osteotomy
• In hinged abduction deformity.
• Occurs when the deformed femoral head fails to slide within the acetabulum
• Raney et al. described Valgus subtrochanteric osteotomy for malformed femoral heads with hinge abduction
• Catterall III and IV with previous failed treatment
• 5-year follow-up, 62% had satisfactory results
• Valgus extension osteotomy- deformity is fixed with a pediatric screw and side plate to relieve this obstruction
VALGUS FLEXION INTERNAL ROTATION OSTEOTOMY
• For Functional retroversion rather than femoral anteversion
• Along with osteotomy simultaneous acetabuloplasty done
• Corrects the functional coxa vara and hinge abduction (valgus osteotomy)
• Establishes a more normal articulation b/w femoral head and the acetabulum
• Corrects external rotation deformity of the distal limb
• Improves joint congruity
OSTEOCHONDROPLASTY (CHEILECTOMY)
• Hip arthroscopy and surgical dislocation of the hip
• For treat certain types of femoral acetabular impingement (FAI) and other intraarticular lesions
• Osteochondroplasty of the hip for FAI (cam and pincer lesions), loose bodies, and chondral and osteochondral defects (OCDs)
Shelf Procedure
• Staheli Osteotomy
• Done in patients with insufficient remodeling capacity
• Bone graft placed just above the hip joint
• Creates a wider roof / shelf over the acetabulum
• Keeps the femoral head from sliding up and out of the socket
• Simple to perform (mini-incision with or without a dry arthroscope)
Chiari Pelvic Osteotomy
• Medial displacement osteotomy that uses cancellous bone with interposed capsule for articulating surface
• Augmented with a shelf procedure
Trochanteric overgrowth
Growth of proximal femur occurs
• Longitudinally towards neck and head
• Vertically to greater trochanter
In Perthes disease
• longitudinal growth is arrested but greater trochanter continues to grow
Trochanteric Advancement
Wagner method of Trochanteric advancement
Macnicol and Makris method
Newer strategies
• Anti-resorptive therapy
• RANK-L inhibitor — Denosumab (inhibits osteoclast formation)
• Bisphosphonates (Decrease osteoclast activity)
• Bone anabolic therapy to stimulate new bone formation
• Intraosseous administration of bisphosphonates
Prognosis
Prognosis is poor if
• Age over 10 years
• Female Sex
• Degree of head involvement (Caterall & Thompson)
• 2+ Head at risk signs
• Herring C at fragmentation stage
• Premature physeal closure
• Restricted ROM
• Increased weight


Leave a Reply