Introduction
-
Pelvic fractures account for less than 5 percent of all skeletal injuries.
-
They are clinically significant due to the high risk of severe hemorrhage.
-
Approximately 10 percent of patients have associated visceral injuries, with an overall mortality rate of about 10 percent.
-
In patients younger than 35 years, pelvic fractures are more commonly seen in females than males.
Surgical Anatomy
-
The pelvic ring consists of two innominate bones and the sacrum.
-
Anterior articulation occurs at the symphysis pubis, while posterior articulation occurs at the sacroiliac joints.
-
The pelvic ring transmits body weight from the trunk to the lower limbs.
-
It also provides protection to pelvic viscera, major blood vessels, and neural structures.
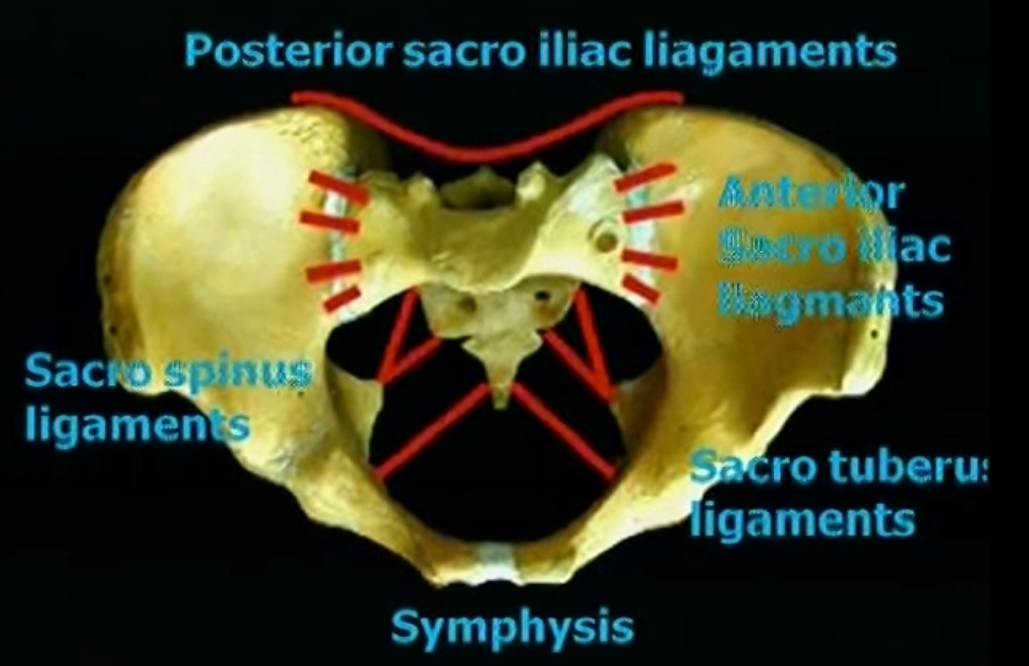
Pelvic Stability
-
Anterior pelvic stability is primarily provided by the sacroiliac ligaments and the iliolumbar ligaments.
-
Posterior pelvic stability is maintained by:
-
Posterior sacroiliac ligaments
-
Sacrococcygeal ligaments
-
Sacrotuberous ligaments
-
Sacrospinous ligaments
-
-
Stability at the symphysis pubis is provided by the superior pubic ligament and the arcuate pubic ligament.
-
Major branches of the common iliac arteries and veins course within the pelvis between the level of the sacroiliac joint and the greater sciatic notch.
Clinical Assessment
-
A pelvic fracture should be suspected in any patient with multiple traumatic injuries.
-
Clinical signs may include swelling and bruising of:
-
Lower abdomen
-
Thighs
-
Perineum
-
Scrotum or vulva
-
-
Abdominal guarding or tenderness suggests possible intraperitoneal bleeding.
-
Repeated manipulation or assessment of an unstable pelvis can disrupt formed clots and worsen hemorrhage.
-
Bladder rupture should be suspected in patients who do not void or in whom the bladder is not palpable after adequate fluid resuscitation.
-
Bladder rupture may be intraperitoneal or extraperitoneal.
-
Intraperitoneal rupture may be associated with massive hemorrhage.
-
-
A detailed neurological examination is required to assess potential injury to the lumbosacral plexus.
Imaging Evaluation
-
An anteroposterior radiograph of the pelvis should be systematically evaluated by dividing the pelvis into 5 zones:
-
Sacroiliac joint region for diastasis or sacral fracture
-
Ilium for fractures
-
Teardrop region, representing the non-articular floor of the acetabulum, for acetabular fractures
-
Obturator foramen for superior or inferior pubic ramus fractures
-
Symphysis pubis for fracture or diastasis
-
-
Inlet view
-
Provides an axial view of the sacrum and sacroiliac joints
-
-
Outlet view
-
Provides a true anteroposterior view of the sacrum and pubic symphysis
-
-
Judet views
-
Obtained at 30 degrees obliquity
-
Obturator oblique view demonstrates the anterior column of the acetabulum
-
Iliac oblique view demonstrates the posterior column and anterior wall of the acetabulum
-
-
Six radiographic lines assist in diagnosing acetabular fractures:
-
Anterior wall of the acetabulum
-
Posterior wall of the acetabulum
-
Roof or dome of the acetabulum
-
Iliopectineal line, corresponding to the anterior column
-
Ischiopectineal line
-
Teardrop
-
Mechanism of Injury
-
Pelvic fractures are broadly classified based on energy transfer:
Low-Energy Injuries
-
Sudden muscular contractions causing avulsion injuries in young athletes
-
Low-energy falls
-
Saddle-type injuries, such as those sustained during motorcycle riding or horse riding
High-Energy Injuries
-
Motor vehicle collisions
-
Pedestrian struck injuries
-
Motorcycle accidents
-
Falls from height
-
Crush injuries
Stress Fractures of the Pelvis
-
Pubic ramus fractures are common in osteoporotic bone.
-
Magnetic resonance imaging is useful for diagnosing posterior pelvic insufficiency fractures.
-
Stress fractures may be seen in the superior and inferior pubic rami, particularly in slim individuals and long-distance runners.
-
Patients typically present with groin pain lasting weeks to months.
-
Initial radiographs may be normal, with fractures becoming more apparent during callus formation.
-
Vitamin D levels should be evaluated to exclude deficiency.
-
Most patients heal with rest and activity modification.
-
Rarely, painful nonunion may persist and require surgical intervention.
Classification of Pelvic Ring Injuries
-
Pelvic fractures are commonly classified using:
-
Young and Burgess classification, based on mechanism of injury
-
Tile classification, based on pelvic stability
-
-
The mechanism-based classification predicts injury severity and blood loss.
-
Stability-based classification guides the need for operative fixation.
Young and Burgess Classification
Anteroposterior Compression Injuries
-
Caused by a front-on force transmitted through the pelvis.
-
Initial injury occurs at the symphysis pubis, followed by posterior sacroiliac disruption with increasing force.
-
Common in motorcyclists and horse riders.
-
Associated with external rotation of both hemipelves.
-
Anteroposterior Compression Type 1
-
Symphyseal widening less than 2.5 centimeters
-
-
Anteroposterior Compression Type 2
-
Symphyseal widening greater than 2.5 centimeters with anterior sacroiliac joint widening
-
Posterior sacroiliac ligaments remain intact
-
-
Anteroposterior Compression Type 3
-
Symphyseal widening greater than 2.5 centimeters with complete sacroiliac joint disruption
-
Lateral Compression Injuries
-
Most common mechanism of pelvic injury.
-
Result from force applied from the side of the pelvis.
-
Common in pedestrians struck by vehicles and side-impact collisions.
-
Lateral Compression Type 1
-
Pubic ramus fracture with ipsilateral anterior sacral alar fracture
-
-
Lateral Compression Type 2
-
Pubic ramus fracture with ipsilateral posterior iliac fracture dislocation
-
-
Lateral Compression Type 3
-
Ipsilateral lateral compression injury with contralateral anteroposterior compression pattern, also known as a windswept pelvis
-
Vertical Shear Injuries
-
Usually occur after a fall from height landing on one leg.
-
Characterized by vertical displacement of one hemipelvis.
-
Involve complete disruption of:
-
Symphysis pubis
-
Sacrotuberous ligaments
-
Sacrospinous ligaments
-
Sacroiliac ligaments
-
Tile Classification
-
Assesses pelvic stability and guides treatment decisions.
-
Type A
-
Stable pelvic fractures
-
-
Type B
-
Rotationally unstable but vertically stable fractures
-
-
Type C
-
Rotationally and vertically unstable fractures
-
Pelvic Binders
-
Pelvic binders should be applied at the level of the greater trochanters, not at the iliac crest.
-
They reduce pelvic volume and provide temporary stabilization.
-
Ideally, binders should not be left in place for more than 24 hours due to the risk of pressure sores.
Angiography and Embolization
-
Immediate transfer for angiography is indicated in ongoing hemorrhage.
-
Selective embolization effectively controls arterial bleeding.
-
Common bleeding sources include the internal iliac artery and superior gluteal artery.
Preperitoneal Pelvic Packing
-
An external fixator is applied initially.
-
The pelvis is accessed using the Stoppa approach.
-
The rectus abdominis muscle is divided in the midline.
-
At least 6 large abdominal packs are inserted:
-
3 on each side of the midline
-
Positioned posteriorly, mid-pelvis, and anteriorly
-
Nonoperative Management
Indications
-
Most lateral compression type 1 and anteroposterior compression type 1 injuries
Relative Indications for Surgery
-
Symphyseal widening greater than 2.5 centimeters
-
Leg-length discrepancy greater than 1.5 centimeters
-
Rotational deformity
-
Sacral displacement greater than 1 centimeter
-
Intractable pain
External Fixation
-
Commonly used as a temporary stabilization method.
-
Can serve as definitive fixation for anterior pelvic injuries.
-
Typically involves insertion of 2 to 3 pins of 5 millimeters diameter along the anterior iliac crest.
-
Supra-acetabular pin placement in the anteroposterior direction may be used, known as the Hanover frame.
-
Contraindicated in acetabular fractures and iliac wing fractures.
-
Vertically unstable fractures may require ipsilateral distal femoral skeletal traction.
-
Temporary posterior stabilization devices, such as the Ganz clamp or Browner fixator, may be used during resuscitation.
Internal Fixation
-
Symphyseal diastasis is treated with plate fixation if there is no open injury or cystostomy tube.
-
Sacral fractures may be treated with plate fixation or sacroiliac screw fixation.
-
Iliac wing fractures are treated with open reduction and internal fixation using lag screws and neutralization plates.
-
Unilateral sacroiliac dislocations are treated with cancellous screw fixation or anterior sacroiliac plating.
-
Bilateral posterior instability requires fixation of the displaced hemipelvis to the sacral body using posterior screw fixation.
Treatment Based on Tile Classification
-
Type A
-
Protected weight bearing and symptomatic treatment
-
-
Type B1 (Open book injuries)
-
Symphyseal diastasis up to 2 centimeters managed with external fixation or symphyseal plating
-
-
Type B2 and B3 (Lateral compression injuries)
-
Ipsilateral injuries usually require no stabilization
-
Contralateral bucket-handle injuries with leg-length discrepancy greater than 1.5 centimeters require external fixation or open reduction and internal fixation
-
-
Type C
-
Managed with external fixation with or without skeletal traction, or definitive open reduction and internal fixation
-
Bowel Injury
-
Rectal or anal perforations caused by bony fragments are considered open fractures and treated accordingly.
-
Rarely, bowel entrapment at the fracture site may cause gastrointestinal obstruction.
-
Presence of bowel injury mandates diverting colostomy.
Postoperative Care
-
Aggressive pulmonary care with incentive spirometry should be initiated early.
-
Early mobilization is encouraged where stability permits.
-
Thromboembolism prophylaxis includes:
-
Elastic stockings
-
Sequential compression devices
-
Pharmacological prophylaxis when hemodynamically appropriate
-
Complications
-
Infection rates range from 0 to 25 percent.
-
Thromboembolic events
-
Malunion, which is rare
-
Nonunion, rare and more commonly seen in young patients
Mortality
-
Hemodynamically stable patients: approximately 3 percent
-
Hemodynamically unstable patients: approximately 38 percent
-
Lateral compression injuries: head injury is the most common cause of death
-
Anteroposterior compression injuries: pelvic and visceral injuries are the leading causes of death
-
Vertical shear injuries: mortality rate approximately 25 percent

Leave a Reply