Courtesy: Dr A Gomoll, Ashok Shyam TV, Ortho
Clinical Context
-
First-time patellar dislocators traditionally require surgery only when a loose body is present.
-
However, many patients present with:
-
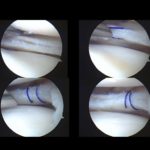
Cartilage defects on magnetic resonance imaging.
-
No loose body.
-
Unclear indication for surgery.
-
Key question:
When should patellofemoral cartilage defects be treated surgically?
Incidence of Patellofemoral Cartilage Defects
-
Patella is the second most common location for cartilage defects after the medial femoral condyle.
-
Cartilage defects are extremely common.
-
Not every defect is symptomatic.
-
Not every anterior knee pain is structural.
Important principle:
Treat the patient, not the MRI.
Defects That Can Often Be Ignored
1. Small Defects Without Pain
-
Patient has instability.
-
Small cartilage lesion.
-
No mechanical symptoms.
-
Management: Address instability; cartilage may not need intervention.
2. Inferomedial Patellar Facet Defects
-
Classic location after patellar dislocation.
-
Inferomedial pole injury from impact.
-
Rarely heavily loaded during normal motion.
-
Often asymptomatic long-term.
-
Management:
-
Remove loose body if present.
-
Focus on instability.
-
Cartilage repair often unnecessary.
-
3. Very Anterior Lateral Femoral Condyle Defects (Countercoup Injury)
-
Occurs during dislocation event.
-
Located outside primary weight-bearing zone.
-
Does not articulate in functional flexion.
-
Management:
-
Debridement if needed.
-
No formal cartilage reconstruction.
-
4. Inferolateral Patellar Defects in Maltracking Patients Undergoing Osteotomy
-
Tibial tubercle osteotomy unloads the inferior patella.
-
If unloading corrects biomechanics, cartilage procedure may not be required.
Defects That Should Be Treated
1. Acute Osteochondral Fractures
-
Young patients.
-
Large fragment.
-
Intact cartilage surface.
-
Treatment:
-
Repair whenever possible.
-
Screws, bioabsorbable darts, or sutures.
-
Better healing in skeletally immature patients.
-
2. Cartilage-Only Delamination in Young Patients
-
Open growth plates.
-
Even without bone attached.
-
Evidence suggests reasonable healing potential.
-
Prefer repair in young patients.
3. Large Chronic Defects in Weight-Bearing Zones
-
Especially involving:
-
Median ridge of the patella.
-
Central or weight-bearing lateral femoral condyle.
-
-
Often associated with:
-
Recurrent instability.
-
Maltracking.
-
These may require:
-
Cartilage restoration.
-
Combined stabilization procedure.
Age Considerations
Skeletally Immature Patients
-
Higher healing potential.
-
Favor repair even if cartilage-only fragment.
-
Combine with MPFL reconstruction if instability present.
Adults (25–30 years and older)
-
Cartilage-only fragments less likely to heal.
-
Fragmented or degenerative pieces:
-
Remove.
-
Consider reconstruction based on size and symptoms.
-
Repair Techniques
Fixation Options
-
Headless compression screws.
-
Bioabsorbable darts.
-
Suture fixation.
-
Open or arthroscopic approaches.
Small studies show:
-
Good healing rates in young patients.
-
Particularly effective in osteochondral fragments.
Reconstruction Options
Used when repair is not possible.
Surface-Based Treatments (Bone Intact)
-
Autologous chondrocyte implantation.
-
Minced autologous cartilage technique.
-
Microfracture (limited role in patella).
-
Bone marrow–augmented cartilage repair.
Osteochondral Techniques (Bone Compromised)
-
Osteochondral autograft.
-
Osteochondral allograft.
Modern Technique: Minced Autologous Cartilage
-
Cartilage biopsy harvested.
-
Minced into small fragments.
-
Mixed with bone marrow aspirate concentrate and fibrin glue.
-
Placed into defect.
-
More cost-efficient than autologous chondrocyte implantation.
-
Increasingly popular option.
Clinical Case Patterns
Case 1: Multiple Dislocations in Adolescent
-
Extensive lateral femoral condyle damage.
-
Required:
-
MPFL reconstruction.
-
Autologous chondrocyte implantation.
-
Guided growth procedure for valgus alignment.
-
Lesson:
Repeated instability leads to progressive cartilage loss.
Case 2: Weight-Bearing Lateral Femoral Condyle Defect
-
Moderate trochlear dysplasia.
-
Osteochondral allograft.
-
MPFL reconstruction.
-
Good integration.
Decision-Making Algorithm
Ignore:
-
Small, non-weight-bearing defects.
-
Inferomedial patella defects.
-
Very anterior lateral femoral condyle lesions.
-
Defects that will be unloaded by osteotomy.
Repair:
-
Large osteochondral fragments.
-
Young patients with viable cartilage.
-
Acute injuries.
Reconstruct:
-
Large defects.
-
Non-repairable fragments.
-
Weight-bearing surface involvement.
-
Median ridge involvement.
-
Chronic recurrent instability cases.
Key Principles
-
Not every cartilage defect needs surgery.
-
Symptoms must correlate with lesion location.
-
Young patients deserve aggressive preservation.
-
Address instability simultaneously.
-
Prevent repeated dislocations to avoid cumulative cartilage damage.
Final Take-Home Points
-
Inferomedial patellar defects: usually ignore.
-
Anterior lateral femoral condyle defects: often ignore.
-
Large fragments: repair if possible.
-
Large chronic defects: reconstruct.
-
Combine cartilage surgery with instability correction.
-
Do not allow repeated dislocations in young patients.

Leave a Reply