Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Current Concepts in Patellar Tendinopathy
- Also known as JUMPER’S KNEE
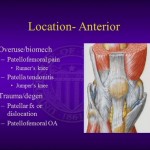
ETIOLOGY-Multifactorial
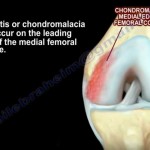
- chronic, repeated stress to the posterior fibers of the tendon, particularly near the inferior pole of the patella.
- increased stress-drives fibroblasts -stimulate prostaglandin E2 and leukotriene B4- lead to tendinopathy
INTRINSIC FACTORS
- laxity, weight, strength and flexibility of the quadriceps and hamstrings,
- Abnormal arch height of the foot.
- leg length difference,
- waist-to-hip ratio,
- vertical jump performance
EXTRINSIC FACTORS
- Excessive training volume and frequency,
- environmental conditions such as irregularities on the ground,
- inappropriate footwear choices
Histology
- Absence of inflammatory cells. !
Instead,
- neovascular proliferative changes
- hypercellularity with atypical fibroblasts resulting in abnormal collagen distribution
Symptoms
- pain at the proximal insertion of the patellar tendon during athletic activities
- less frequently at the tibial insertion.
- Pain is typicall triggered by running, jumping, crouching,
duration of symptoms
- acute (less than 6 weeks),
- subacute (6 to 12 weeks),
- chronic (more than 3 months).
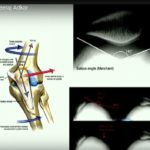
Diagnosis and evaluation
- accurately pinpoint the location of pain
Basset sign
- “passive extension—flexion sign”
- patient is lying down
- palpating the anterior aspect of the fully extended knee
- identifying the tender point (typically at the inferior pole of the patella and proximal part of the patellar tendon)
- A positive test is indicated by reduced tenderness on palpation as the knee is flexed to 90°
Standing Active Quadriceps Sign
- the patient is standing on both extremities
- palpating the entire patellar tendon
- repeat the test with the patient standing only on the affected extremity with 30° of knee flexion.
- If pain significantly lessens in the latter position, the test is considered positive.
INVESTIGATIONS
- Radiographs- overall view of the joint , rule out significant bony involvement or concomitant disorders
Ultrasound
- provides detailed visualization of the tendon
- focal tendon thickening,hypoechogenicity,increased extracellular fluid
MRI
- intrasubstance edema in the tendon
- In chronic cases-reveal cortical irregularities affecting the inferior patellar pole
Blazina Classification
- I -Pain after sports activity
- II -Pain at the beginning of activity, disappearing after warming up, and reappearing at the end of the activity
- III -Pain during and after activity with the patient being unable to participate in sports
- IV -Complete tendon rupture
TREATMENT- Conservative Management
- Eccentric and isometric exercises (45 min )
- patellar strapping (2 hours)
- sports taping (2 hours)
- platelet-rich plasma (PRP) injections- optimal infiltration site –
- autologous whole-blood injections
- dry needling
- Steroid injections-not advised; potential risk of tendon rupture
- Emerging therapeutic alternatives–Ultrasound-guided percutaneous needle tenotomy (PNT) with a well-structured rehabilitation program
SURGICAL OPTIONS
Open Surgery
involves:
- making a 5-cm longitudinal incision on the midline of the patellar tendon,
- carefully dissecting the paratenon,
- Performing a posterior central tenotomy to expose the deepest layers of the tendon
- complete the debridement,
- drilling multiple holes in the inferior pole of the patella
- Direct suture of the tendon.
Arthroscopic Surgery
- introduced by Johnson,
- excision of 25% to 30% -nonarticular portion of the inferior patellar pole – a 5-mm spherical arthroscopic burr.
- both open and arthroscopic surgical approaches- favorable success rates .
- arthroscopic treatment may lead to faster Return to sports..
the use of ultrasound guidance with Doppler during arthroscopic surgery -valuable resource
RECENT DEVOLOPMENT-collagen-based bioinductive patch and a PRP membrane in addition to an intratendinous leukocyte-rich PRP injection.

Leave a Reply