Courtesy: Dr Kunal Kalra
Children’s Hospital of Michigan Pediatric Emergency Department, Michigan, USA
www.chmpem.com
Introduction
- Increasing incidence of ACL injuries in children and adolescents.
- Historically managed nonoperatively due to fear of physeal damage.
- Modern shift toward early surgical intervention due to high rates of instability and secondary injuries with conservative care.
- The article focuses on anatomical, diagnostic, and surgical considerations in treating skeletally immature patients.
Applied Anatomy
- ACL provides anterior and rotational stability.
- Rapid growth during childhood and adolescence:
- Length increases from ~18.4 mm (age 1) to ~35.7 mm (age 15).
- The ACL lies close to growth plates, especially the distal femoral and proximal tibial physes.
Anatomical changes with age:
- ACL becomes more vertical as the child matures.
- Tibial attachment migrates posteriorly.
Assessment of Skeletal Maturity
Vital for surgical planning.
Methods:
- Chronologic age (inaccurate alone)
- Tanner staging (pubertal development)
- Greulich & Pyle atlas (hand radiograph)
- Knee MRI for growth plate status
Classification:
- Prepubescent: >2 years growth remaining – Physeal-sparing
- Pubescent: 1–2 years growth remaining – Physeal-respecting
- Skeletally mature: <1 year growth -Transphyseal (adult-type)
Risk Factors for ACL Injury
Nonmodifiable:
Female sex, younger age, narrow intercondylar notch, increased tibial slope.
Modifiable:
- Poor neuromuscular control
- Early sport specialization
- Inadequate strength/balance training
- Female athletes in pivoting sports are at higher risk.
Nonoperative vs Operative Management
Nonoperative treatment associated with:
- 75% rate of instability
- High rates of meniscal/chondral damage
- Delayed surgery leads to worse outcomes
- Early operative treatment is now preferred to prevent joint degeneration.
ACL Repair
- BEAR (Bridge-Enhanced ACL Repair): biological scaffold repair technique
- Promising in adults but has high failure rates in children.
- Not recommended as standard treatment for skeletally immature patients.
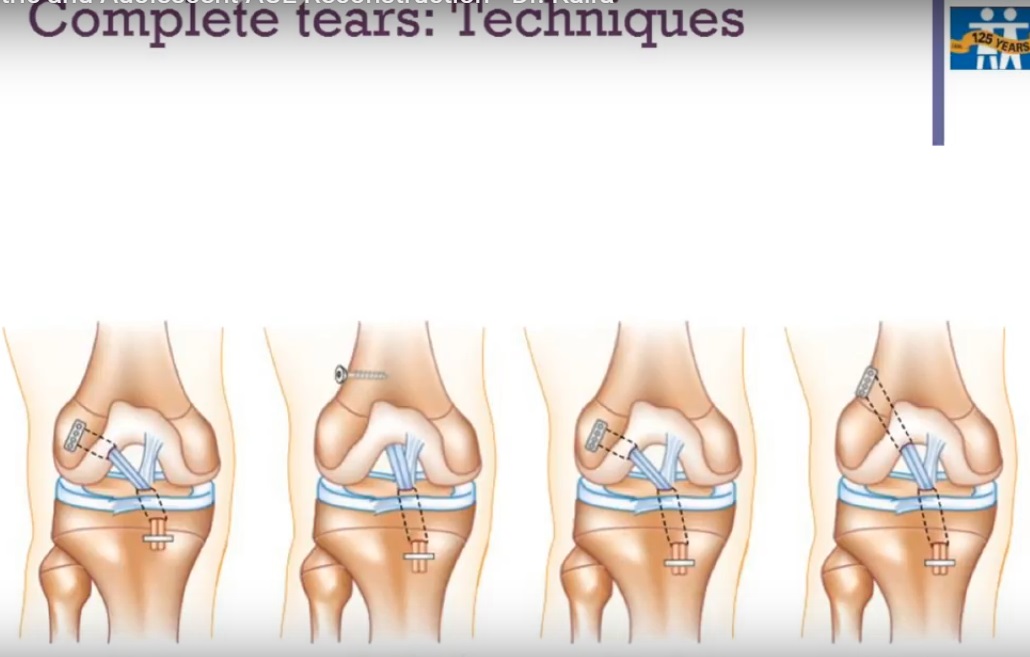
ACL Reconstruction Techniques
-Physeal-Sparing
- ITB Over-the-Top (Kocher–Micheli):
- No tunnels or hardware
- Best for children <11 years
-All-Epiphyseal:
- Epiphyseal tunnels only
- Anatomic but technically demanding
-Physeal-Respecting
- Partial Transphyseal:
- Tibial tunnel only crosses physis
- Femoral tunnel epiphyseal or over-the-top
Full Transphyseal:
- Both tunnels through growth plates
- Safe in older adolescents with precautions
Graft Selection
Preferred:
- Hamstring tendon: widely used, size-dependent
- Quadriceps tendon: growing popularity, larger size, low morbidity
- ITB autograft: best for young children, used in over-the-top reconstructions
Avoid:
- BTB (bone-patellar tendon-bone): bone plugs can arrest growth
- Allografts: high failure rates in active 10 mm: ~2.1%
- Prevention: small tunnels, soft-tissue grafts, fluoroscopy-guided technique, avoid screws across physes
Concomitant Procedures
Lateral Extra-articular Tenodesis (LET):
- Reduces rotational stress on the ACL graft
- Beneficial in high-risk patients: pivoting athletes, hyperlaxity
- Safe when fixed distal to the femoral physis
Growth Modulation
- Temporary hemiepiphysiodesis with plates/screws to correct/prevent deformity
- Especially in patients with valgus deformity or mechanical axis deviation
Prevention Programs
Focused on:
- Neuromuscular training
- Plyometrics
- Balance and strength training
- Best results in female athletes 11–18 years
- Proven to reduce ACL injury rates by 52–88% when implemented properly
Programs:
- FIFA 11+
- PEP
- KIPP
Conclusion
- Pediatric ACL injuries require individualized, growth-sensitive management.
- Early reconstruction is preferred over nonoperative care.
- Surgical technique selection depends on skeletal maturity.
- Physeal-sparing for younger, transphyseal acceptable in near-mature adolescents.
- LET and growth modulation improve outcomes in select patients.
- Prevention programs are essential, especially for young female athletes.
Leave a Reply