Courtesy: Dr Alan Getgood, Ashok Shyam, Ortho TV
Introduction
-
The session focuses on practical concepts in knee osteotomy, using real clinical cases to illustrate decision-making.
-
Osteotomy remains an important procedure for young, active patients with malalignment and compartmental knee pathology.
-
Revisiting fundamental principles is valuable because:
-
These procedures can be technically demanding.
-
Proper patient selection and planning significantly influence outcomes.
-
-
Many modern surgeons were strongly influenced by earlier pioneers in osteotomy techniques whose contributions helped shape current practices.
Case 1: Active Patient with Medial Compartment Pain
Patient Profile
-
43-year-old female.
-
Very active lifestyle; works as a spin class instructor.
-
Bilateral mild varus limb alignment.
-
Good quadriceps strength and muscle bulk.
-
Medial joint line tenderness.
Patient Expectations
-
Wishes to avoid joint replacement.
-
Goal is rapid return to high activity level.
Imaging and Alignment
-
Radiographs show medial compartment degeneration.
-
Alignment films reveal mild varus deformity.
Key Considerations
-
Determine whether deformity originates from:
-
Tibia
-
Femur
-
-
Small corrections may be treated with tibial osteotomy, depending on surgeon preference.
Osteotomy Options
Tibial Osteotomy
Advantages:
-
Corrects alignment across the entire knee flexion arc.
-
Particularly useful for activities involving flexion such as:
-
Cycling
-
Skiing
-
Horse riding
-
Femoral Osteotomy
Characteristics:
-
Primarily affects early knee flexion range.
Leg Length Consideration
Important principle:
-
Opening wedge osteotomy lengthens the limb.
-
Closing wedge osteotomy shortens the limb.
Guideline:
-
If limb is already long – consider closing wedge osteotomy.
-
If limb is short – consider opening wedge osteotomy.
Ignoring limb length differences can lead to postoperative dissatisfaction.
Role of MRI
Possible indications:
-
Evaluate for meniscal or chondral pathology.
-
Assess lateral compartment condition.
However:
-
In health systems with limited resources, MRI may not be routinely required when radiographs clearly show osteoarthritis.
Treatment Performed
-
Bilateral high tibial osteotomy
-
Small correction (~6 mm).
-
Fixation with locking plate system.
Rehabilitation
Typical protocol:
-
Initial partial weight bearing.
-
Gradual progression to full weight bearing.
Outcome example:
-
Patient resumed teaching spin classes within six weeks.
Osteotomy Gap Management
Bone Grafting Debate
For small corrections (<10 mm):
-
Many surgeons do not graft.
For larger corrections:
-
Bone graft or substitute may be used.
Common materials:
-
Allograft chips
-
Autograft bone
-
Bone substitutes
Purpose of grafting:
-
Fill the osteotomy gap.
-
Improve stability and reduce bleeding.
-
Not necessarily required for union in small gaps.
Protecting the Lateral Hinge
Techniques to Prevent Hinge Fracture
Important steps include:
-
Correct osteotomy placement.
-
Complete posterior cortex release.
-
Adequate medial collateral ligament release.
-
Controlled gradual opening.
Methods Used
Possible strategies:
-
Hinge K-wire
-
Lateral hinge screw
-
Controlled spreading instruments
-
Stacked osteotomes
Goal:
-
Achieve controlled plastic deformation rather than sudden fracture.
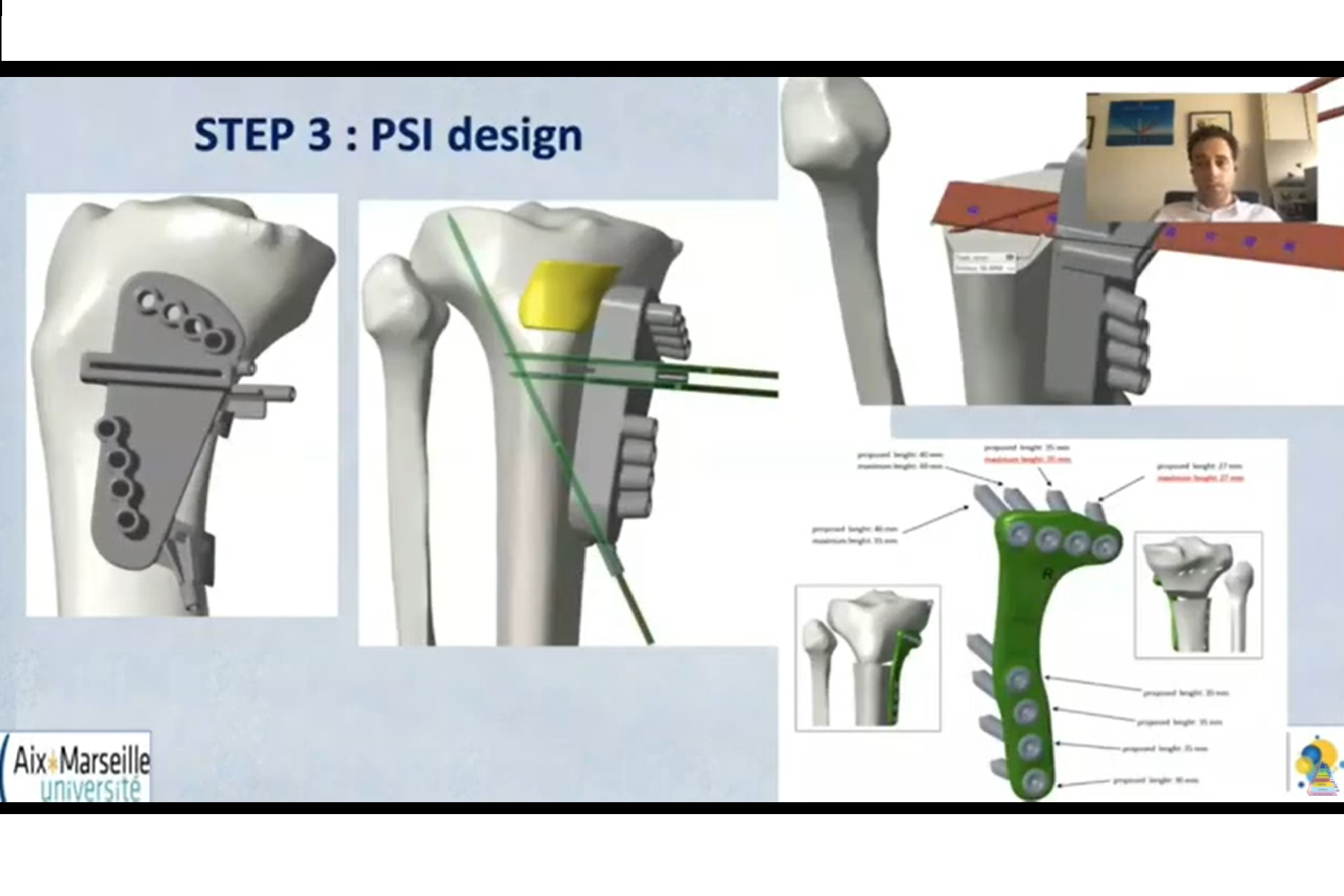
Patient-Specific Instrumentation (PSI)
Advantages
-
Accurate preoperative planning.
-
Reproducible correction.
-
Reduced reliance on intraoperative navigation.
Current Use
Some surgeons use PSI for all osteotomies, while others reserve it for:
-
Complex deformities
-
Small, precise corrections.
Limitations
-
Accurate placement on bone can be challenging.
-
Incorrect positioning may lead to errors.
Pain Management in Osteotomy
Typical Analgesia Strategies
-
Spinal anesthesia
-
Local anesthetic infiltration
-
Peripheral nerve blocks
-
Oral analgesics
Common medications:
-
Opioids
-
NSAIDs
-
Paracetamol
NSAIDs and Bone Healing
Concern:
-
Animal studies suggest possible delayed bone healing.
Clinical practice varies:
-
Some surgeons avoid NSAIDs.
-
Others use them briefly for postoperative pain.
Opioid Considerations
-
Overprescription has contributed to the opioid crisis in some countries.
-
Short courses are usually sufficient for osteotomy patients.
Postoperative Weight Bearing
Protocols vary between surgeons:
Examples include:
-
Partial weight bearing for 4 weeks.
-
Gradual progression to full weight bearing.
Observation:
-
Even when unrestricted weight bearing is allowed, patients usually self-limit due to pain.
Case 2: Young Patient with Lateral Compartment Degeneration
Patient Details
-
29-year-old male.
-
Previous subtotal lateral meniscectomy.
-
Persistent lateral knee pain.
-
Valgus alignment.
Clinical Findings
-
Mechanical symptoms.
-
Stable ligaments.
-
Pain during pivoting movements.
Imaging
-
Early lateral compartment arthritis.
-
Valgus malalignment.
Surgical Planning
Traditional assumption:
-
Lateral OA – distal femoral osteotomy
However:
-
Detailed deformity analysis may reveal tibial-based deformity.
Key message:
-
Always perform full alignment analysis rather than relying on assumptions.
Treatment
-
Closing wedge tibial osteotomy
-
Demonstrated good outcomes for selected patients.
Case 3: Recurrent ACL Failure with Increased Tibial Slope
Clinical History
-
Multiple failed ACL reconstructions.
-
Medial meniscus deficiency.
-
Lateral meniscus root tear.
Key Findings
-
Increased posterior tibial slope (~17°).
-
Increased anterior tibial translation.
Importance of Tibial Slope
Increased posterior slope leads to:
-
Greater anterior tibial translation
-
Increased ACL graft stress
-
Higher risk of reconstruction failure
Surgical Options
Slope-Reducing Osteotomy
Anterior closing wedge osteotomy can:
-
Reduce posterior tibial slope.
-
Improve knee stability.
Staged Approach
Stage 1:
-
Correct tibial slope.
Stage 2:
-
Revision ACL reconstruction if instability persists.
Case 4: Hyperextension Instability
Problem
-
Persistent knee hyperextension after ligament reconstruction.
-
Relatively flat tibial slope.
Treatment Concept
Increase tibial slope using anterior opening wedge osteotomy.
Expected benefits:
-
Reduce hyperextension.
-
Improve PCL stability.
Case 5: Severe Varus Knee with Multiligament Injury
Clinical Situation
-
Traumatic knee dislocation.
-
ACL, PCL, and posterolateral corner injury.
-
Significant varus deformity.
Alignment Strategy
If mechanical axis lies outside the knee joint, consider:
-
Double-level osteotomy
-
Tibial correction
-
Femoral correction
-
Goal:
-
Restore neutral mechanical axis.
Treatment Approach
Stage 1:
-
Correct alignment using osteotomy.
Stage 2:
-
Perform ligament reconstruction.
Key Takeaways
Osteotomy Remains Essential For
-
Young active patients.
-
Malalignment with compartment overload.
-
Ligament instability associated with abnormal bone morphology.
Principles for Success
-
Careful deformity analysis.
-
Understand relationship between alignment and ligament forces.
-
Consider tibial slope in instability cases.
-
Tailor osteotomy type to patient anatomy.
-
Plan staged procedures when necessary.

Leave a Reply