Definition
-
Osteosarcoma is a malignant primary bone tumor defined by the production of osteoid by malignant cells.
-
It is the most common non-hematologic primary malignancy of bone.
Incidence
-
Annual incidence is approximately one to three cases per million population.
-
Occurs worldwide with no significant racial predilection.
Age Distribution
-
Osteosarcoma can occur at any age.
-
Primary high-grade osteosarcoma:
-
Most commonly occurs during the second decade of life.
-
-
Parosteal osteosarcoma:
-
Peak incidence in the third to fourth decades.
-
-
Secondary osteosarcoma:
-
More frequently seen in older adults.
-
Sex Distribution
-
Overall, there is a slight male predominance.
-
Parosteal osteosarcoma shows a female predominance.
Genetic Associations and Predisposing Conditions
-
Most cases are sporadic.
-
Increased risk is associated with:
-
Hereditary retinoblastoma
-
Li–Fraumeni syndrome
-
Rothmund–Thomson syndrome
-
Common Anatomical Sites
-
Typically arises in regions of rapid bone growth.
-
Most frequent locations:
-
Distal femur (most common)
-
Proximal tibia (second most common)
-
Proximal humerus (third most common)
-
-
Majority of lesions originate in the metaphysis of long bones.
Clinical Presentation
-
Progressive pain is the most common presenting symptom.
-
Pain may initially respond to rest or conservative treatment.
-
Night pain occurs in approximately twenty-five percent of patients.
-
Low-grade surface osteosarcomas may present as a painless enlarging mass.
Delay in Diagnosis
-
Average delay in diagnosis is approximately fifteen weeks.
-
Patient-related delay: six weeks
-
Physician-related delay: nine weeks
-
-
Common causes include:
-
Failure to obtain initial radiographs
-
Failure to repeat imaging despite persistent symptoms
-
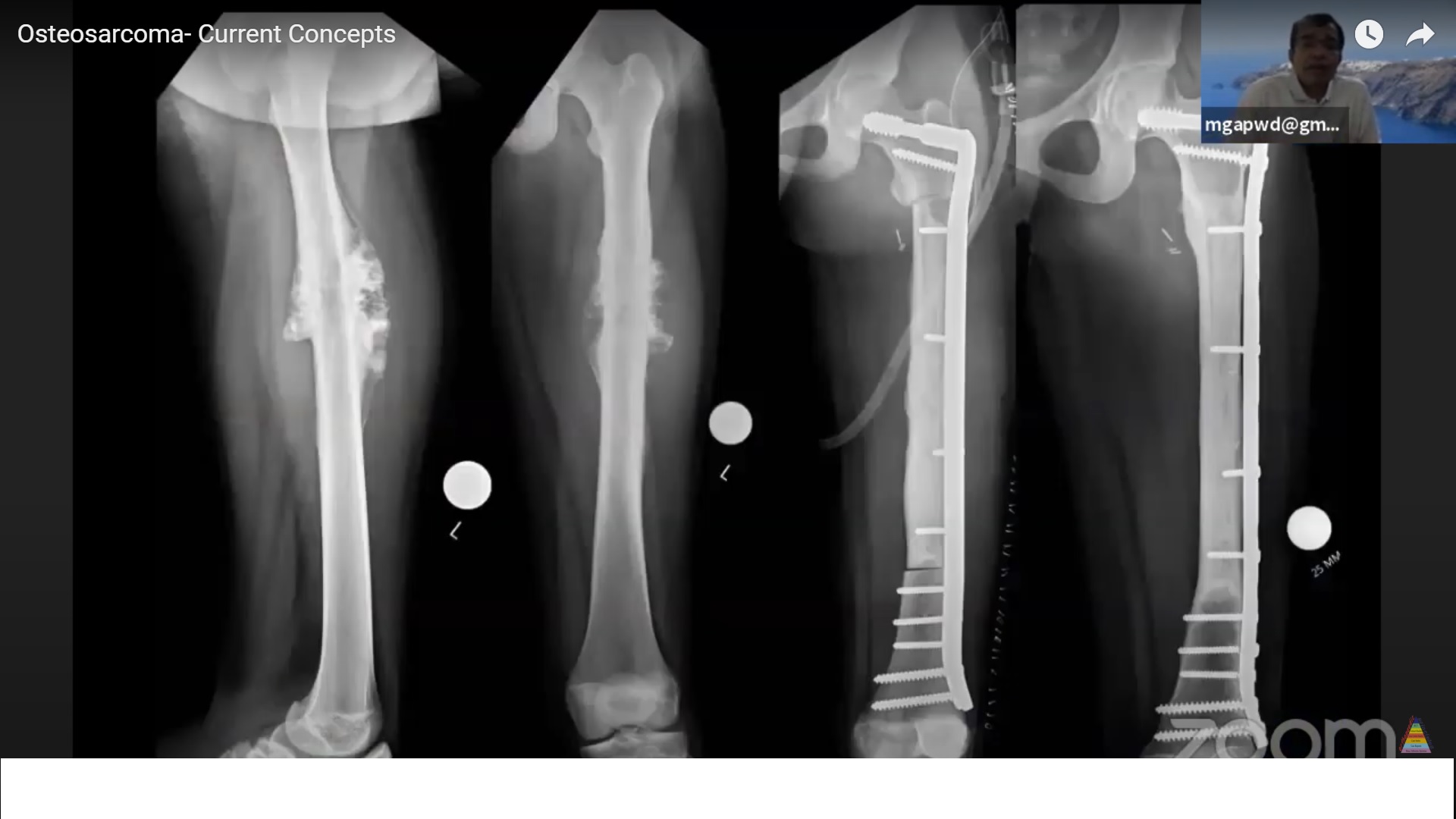
Radiographic Features (Plain Radiographs)
-
Aggressive metaphyseal lesion involving long bones.
-
May appear:
-
Blastic
-
Lytic
-
Mixed
-
-
Poorly defined, permeative margins.
-
Cortical destruction with an associated soft-tissue mass.
-
Periosteal reaction patterns include:
-
Codman triangle
-
Sunburst appearance
-
Hair-on-end appearance
-
Advanced Imaging
-
Magnetic resonance imaging:
-
Best modality for assessing intraosseous extent
-
Evaluates soft-tissue involvement and neurovascular encasement
-
-
Bone scintigraphy:
-
Used to detect skeletal metastases
-
-
Chest radiography and computed tomography:
-
Essential for identifying pulmonary metastases
-
-
All imaging studies should be completed prior to biopsy.
Patterns of Tumor Spread
-
Lungs are the most common site of metastasis.
-
Bone metastases occur less frequently but are associated with worse prognosis.
-
Skip metastases may occur:
-
Within the same bone
-
Across an adjacent joint
-
Classification of Osteosarcoma
Primary Osteosarcoma
-
Conventional osteosarcoma
-
Low-grade intramedullary osteosarcoma
-
Parosteal osteosarcoma
-
Periosteal osteosarcoma
-
High-grade surface osteosarcoma
-
Telangiectatic osteosarcoma
-
Small cell osteosarcoma
Secondary Osteosarcoma
-
Develops in association with a pre-existing condition or insult
Conventional Osteosarcoma
-
Most common subtype.
-
High-grade intramedullary tumor.
-
Frequently breaches the cortex and forms a large soft-tissue mass.
-
Histologic features include:
-
Malignant spindle-shaped cells
-
Definite osteoid production
-
High mitotic activity and marked nuclear pleomorphism
-
Periosteal Osteosarcoma
-
Intermediate-grade malignancy.
-
Arises from the bone surface.
-
Commonly involves the diaphysis of the femur or tibia.
-
Histology shows:
-
Osteoid-producing spindle cells
-
Prominent cartilaginous lobules
-
Low-Grade Intramedullary Osteosarcoma
-
Rare and slow-growing tumor.
-
Can mimic benign conditions such as fibrous dysplasia or osteoblastoma.
-
Located within the medullary cavity.
-
Histology reveals mildly atypical spindle cells producing irregular bone.
Parosteal Osteosarcoma
-
Low-grade surface osteosarcoma.
-
Typically arises from the posterior aspect of the distal femur.
-
Appears as a densely ossified, lobulated mass.
-
Computed tomography helps differentiate it from:
-
Myositis ossificans
-
Osteochondroma
-
High-Grade Surface Osteosarcoma
-
Least common subtype.
-
Highly aggressive tumor originating from the bone surface.
-
Medullary canal involvement is common at presentation.
-
Histology resembles high-grade conventional osteosarcoma.
Telangiectatic Osteosarcoma
-
Purely lytic and often expansile lesion.
-
Radiographically mimics aneurysmal bone cyst.
-
Grossly consists of blood-filled cystic spaces.
-
Microscopy demonstrates malignant cells within fibrous septa.
Small Cell Osteosarcoma
-
High-grade malignancy composed of small round blue cells.
-
Radiographically and histologically mimics Ewing sarcoma or lymphoma.
-
Diagnosis often requires immunohistochemistry and cytogenetic analysis.
Secondary Osteosarcoma
-
Arises in association with:
-
Paget disease of bone (one to ten percent risk)
-
Prior radiation therapy exceeding two thousand five hundred centigray
-
-
Common anatomical sites:
-
Pelvis
-
Spine
-
Skull
-
Ribs
-
Scapula
-
-
Latency period typically ranges from ten to fifteen years after radiation exposure.
Prognosis: Historical and Modern Outcomes
-
Prior to the use of chemotherapy:
-
Approximately eighty percent mortality within two years
-
-
With modern multimodal treatment:
-
Sixty to seventy-five percent survival for high-grade localized disease
-
Approximately ninety percent survival for low-grade osteosarcoma
-
Prognostic Factors
-
Presence and location of metastases are the most important prognostic factors.
-
Pulmonary metastases at diagnosis (approximately fifteen percent):
-
Associated with poor prognosis
-
-
Non-pulmonary metastases:
-
Less than five percent survival
-
-
Tumor grade, size, and anatomical location also influence outcome.
Treatment of High-Grade Osteosarcoma
-
Neoadjuvant chemotherapy
-
Wide or radical surgical resection or amputation
-
Adjuvant chemotherapy
-
Pulmonary metastasectomy when feasible
Histologic Response to Chemotherapy
-
Greater than ninety percent tumor necrosis indicates an excellent prognosis.
-
Poor histologic response is associated with increased risk of relapse.
Treatment of Low-Grade Osteosarcoma
-
Managed with wide surgical resection or amputation alone.
-
Chemotherapy is generally not indicated.
Recurrence and Relapse
-
Approximately fifty percent of high-grade osteosarcomas relapse.
-
Local recurrence rate is approximately ten percent.
-
Local recurrence is associated with a very poor prognosis.
Management of Relapse
-
Radical amputation when curative intent is pursued.
-
Additional chemotherapy.
-
Pulmonary metastases managed with surgical resection and chemotherapy when possible.
Poor Prognostic Factors After Relapse
-
Early relapse after completion of initial treatment.
-
Eight or more pulmonary nodules.
-
Pulmonary nodules larger than three centimeters.
-
Unresectable pulmonary metastases.

Very nice