Courtesy: Dr Amr Abdelgawad,
Texas Tech University, El Paso, USA
Osteoid Osteoma in Children: Pathology, Imaging, and Management
Overview
- Osteoid osteoma is a benign bone forming tumor commonly seen in children and young adults.
- It is characterized by a small central nidus surrounded by reactive sclerotic bone.
- The lesion most often affects long bones and occasionally involves the spine.
Pathology
- Osteoid osteoma consists of two main components: the nidus and the surrounding reactive bone.
- The nidus is composed of immature woven bone trabeculae within a fibrovascular stroma.
- The surrounding host bone develops dense reactive sclerosis in response to the nidus.
- The nidus is typically less than one point five centimeters in diameter.
Epidemiology
- The condition commonly occurs during the second and third decades of life.
- It is more frequent in males than females.
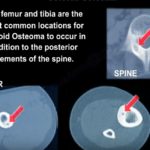
- It often involves the diaphysis of long bones such as the tibia or femur.
- Spinal involvement may occur and can present with painful scoliosis.
Clinical Presentation
- Pain is the most prominent symptom.
- The pain is characteristically worse at night.
- It is typically relieved by nonsteroidal anti inflammatory medication.
- The pain is not significantly relieved by rest.
- In spinal lesions, patients may present with painful scoliosis.
Radiographic Features
- Plain radiographs often show dense cortical sclerosis surrounding the lesion.
- The central nidus may be difficult to identify on radiographs.
- A radiolucent nidus with surrounding sclerosis may be visible on detailed views.
Computed Tomography Findings
- Computed tomography is the most sensitive modality for detecting the nidus.
- It demonstrates a well defined radiolucent nidus surrounded by dense reactive bone.
- The nidus size helps distinguish osteoid osteoma from osteoblastoma.
Magnetic Resonance Imaging Findings
- Magnetic resonance imaging may show surrounding marrow and soft tissue edema.
- The nidus may be less conspicuous than on computed tomography.
Bone Scan
- Bone scintigraphy typically shows intense focal uptake corresponding to the lesion.
Management
- Osteoid osteoma is often self limiting and may resolve over time.
- Initial management may include nonsteroidal anti inflammatory medication for symptom control.
- Surgical excision is an option when symptoms persist.
- Complete removal of the nidus is essential for cure.
- Computed tomography guided radiofrequency ablation is widely used and minimally invasive.
- This technique provides rapid symptom relief when successfully performed.
Special Considerations
- Radiofrequency ablation may not be suitable for lesions near critical neurovascular structures.
- Treatment planning should involve multidisciplinary discussion.
Summary
- Osteoid osteoma is a benign but painful tumor with characteristic imaging findings.
- Accurate diagnosis allows effective minimally invasive treatment with excellent outcomes.


Leave a Reply