Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Osteochondritis Dissecans (OCD) of Knee
OCD is a localized condition where a segment of subchondral bone and its overlying cartilage undergoes avascular necrosis and may separate from surrounding bone.
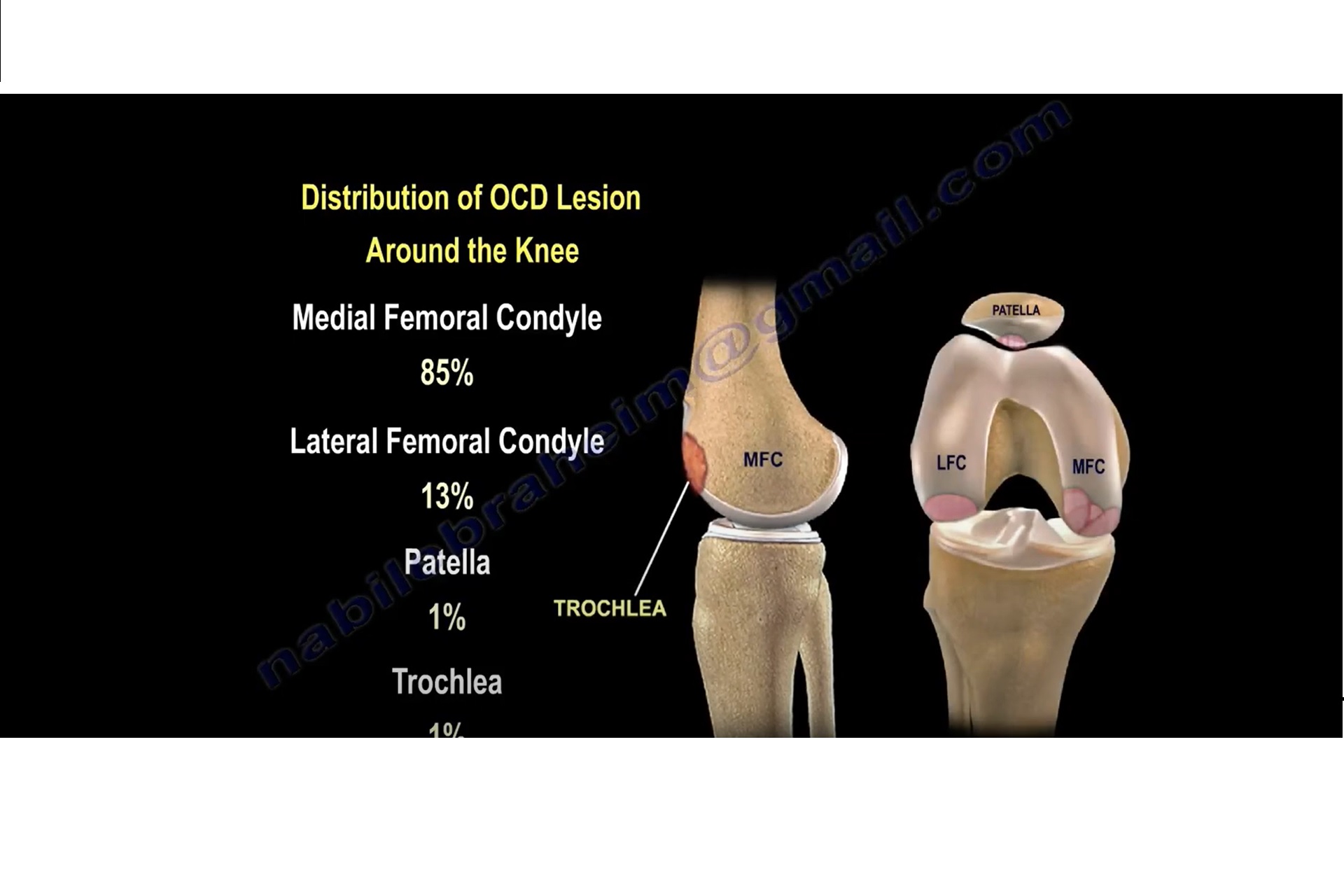
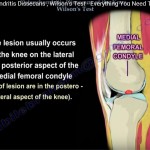
Commonly affects the knee, especially the lateral aspect of the medial femoral condyle.
Etiology And Pathophysiology
- Repetitive microtrauma
- Ischemia/vascular insufficiency
- Genetic and anatomical predisposition
- Cartilage and bone interface disruption
Epidemiology
- Most common in adolescents aged 10–20 years
- Frequently seen in young athletes
Clinical Features
- Pain: Activity-related pain, especially after sports or prolonged standing (Miller, Turek).
- Swelling: Intermittent or persistent joint effusion.
- Mechanical Symptoms: Catching, locking, or giving way due to unstable osteochondral fragments (Campbell, Rockwood).
- Tenderness: Localized tenderness over the lateral aspect of the medial femoral condyle.
- Wilson’s Sign : Pain reproduced with internal rotation of the tibia during knee extension, relieved by external rotation.
- Limp or Altered Gait: Particularly in active adolescents.
- Reduced Range of Motion: In advanced or unstable cases.
- Quadriceps Atrophy: May be seen with chronic involvement.
Classification Systems
Clanton and DeLee Classification:
- Stage I: Depressed osteochondral lesion without fragmentation
- Stage II: Fragment partially detached
- Stage III: Fragment completely detached but remains in place
- Stage IV: Fragment is loose and displaced (loose body)
Hefti MRI Classification:
- Grade I: Small signal changes in subchondral bone
- Grade II: Articular cartilage intact, but a cyst or signal beneath
- Grade III: Articular cartilage breached with high signal interface
- Grade IV: Detached fragment with fluid surrounding lesion
Berndt and Harty Modified (for OCD by MRI):
- Useful for talar dome but adapted for knee
- Helps assess stability and healing potential
Stable vs. Unstable Lesions :
- Stable: Intact articular cartilage, no movement of fragment
- Unstable: Disrupted cartilage, potential for loose body formation
Plain Radiographs:
- Initial modality for suspected OCD.
- Tunnel (intercondylar) view most sensitive for medial femoral condyle lesions (Turek, Rockwood).
- Lateral and AP views may show radiolucent areas, sclerosis, or loose fragments.
MRI:
- Gold standard for early detection and evaluating lesion stability (DeLee & Drez).
- Provides detailed visualization of subchondral bone and overlying cartilage.
- Helps determine size, depth, cartilage breach, and presence of fluid interface (Hefti grade III–IV).
- Essential for staging and treatment planning, especially in skeletally immature patients.
CT Scan:
- Useful for precise assessment of bone fragment morphology and size.
- Beneficial in preoperative planning and evaluating non-union or healed lesions with residual symptoms.
Bone Scan (rarely used):
- Demonstrates increased uptake in active lesions.
- Helps differentiate between viable and necrotic bone, though replaced largely by MRI.
Ultrasound (limited role):
- May detect joint effusion or assist in guiding aspiration/injection but not diagnostic for OCD.
Nonoperative Management
Indications:
- Skeletally immature patients with stable lesions (Campbell, Miller).
- Absence of loose bodies or significant mechanical symptoms.
Conservative Strategy:
Activity Modification: Avoid impact sports and excessive weight-bearing.
Immobilization: May use hinged knee brace or cast in early phases for symptom relief and fragment stability.
Protected Weight-Bearing: Non-weight bearing or partial weight bearing based on symptoms and radiologic stage.
Operative Management
Indications:
- Unstable lesions or failed conservative management
- Symptomatic lesions in skeletally mature individuals
- Presence of mechanical symptoms (locking, catching)
- Loose bodies or cartilage delamination
Drilling (Retrograde or Transarticular):
- Aimed at promoting revascularization and subchondral bone healing.
Retrograde Drilling: Performed from the non-articular bone surface under fluoroscopic or arthroscopic guidance, avoiding cartilage disruption. Suitable for lesions with intact cartilage surface. - Transarticular Drilling: Involves direct perforation through the articular cartilage into the subchondral lesion. More commonly used when cartilage surface is breached.
- Typically done arthroscopically.
Multiple small drill holes (2–3 mm) are made to penetrate sclerotic bone and enhance neovascularization. - Often used in skeletally immature patients with stable lesions unresponsive to conservative therapy.
Minimal morbidity and allows for other procedures (e.g., fixation) if instability is identified intraoperatively.
Internal Fixation:
- Employed for unstable yet viable osteochondral fragments that can be anatomically reduced.
Fixation Devices:
- Metal Screws (e.g., cannulated headless compression screws): Provide rigid fixation but may require later removal.
- Bioabsorbable Pins/Screws: Avoid need for removal; resorb over time.
- Herbert Screws or headless compression screws allow compression without protruding hardware.
Osteochondral Autograft Transfer (OATS):
- Involves transplantation of cylindrical osteochondral plugs (cartilage with underlying bone) from non-weight-bearing areas (typically lateral femoral condyle) to the defect site.
Indications:
- Medium to large-sized symptomatic OCD lesions (typically 1–2.5 cm²).
- Lesions with overlying cartilage damage where fragment salvage is not possible.
- Skeletally mature patients or those with persistent symptoms despite conservative management or fixation.
Surgical Technique:
- Performed via mini-open or arthroscopic-assisted approach.
- Donor plugs are harvested using a coring reamer from non-articulating surface.
- Recipient site is debrided and prepared to match plug size.
- Grafts are press-fit into the defect to restore surface congruity.
- Multiple plugs may be needed for larger lesions (mosaicplasty variation).
Autologous Chondrocyte Implantation (ACI):
- A two-stage cell-based cartilage restoration technique.
Indications:
- Large, symptomatic full-thickness cartilage lesions (>2–4 cm²).
- Failed prior cartilage repair procedures.
- Typically used in younger, active individuals with high functional demands.
Stage 1 – Chondrocyte Harvest:
- Arthroscopic biopsy from non-weight-bearing articular cartilage (usually intercondylar notch or trochlea).
Cells sent to a specialized lab for culture and expansion over several weeks.
Stage 2 – Implantation:
- Performed via open arthrotomy.
- The defect is debrided to healthy cartilage margins.
- Periosteal flap (1st generation) or collagen membrane (2nd/3rd generation ACI) is sutured over the lesion.
- Cultured autologous chondrocytes are injected under the flap or seeded on the membrane prior to implantation.
Generations of ACI:
- First Generation: Uses periosteal flap from tibia (higher hypertrophy risk).
- Second Generation: Uses collagen membrane (e.g., Bio-Gide®).
- Third Generation: Matrix-induced ACI (MACI) – cells seeded onto scaffold matrix prior to implantation.
Mosaicplasty:
- Involves transplantation of multiple small cylindrical osteochondral grafts (cartilage with underlying bone) from non-weight-bearing zones (usually the periphery of the femoral condyle) into the defect.
- Considered a variation of OATS (osteochondral autograft transfer), used when a single large plug is insufficient to fill the lesion.
Indications:
- Medium to large-sized OCD lesions not amenable to fixation.
- Lesions with compromised cartilage surface integrity.
Surgical Technique:
- Performed arthroscopically or via a mini-open approach.
- Multiple grafts (plugs) harvested and inserted in a mosaic-like fashion to recreate joint surface congruity.
- Requires precise alignment and depth matching to minimize step-offs between grafts.
Allograft Transplantation:
Definition:
- Transplantation of fresh osteochondral tissue harvested from a cadaver donor.
- Contains both viable cartilage and subchondral bone.
Indications:
- Large osteochondral lesions not suitable for autograft due to size or location.
- Salvage procedure after failed prior repairs.
- Uncontained or irregular lesions that cannot be adequately treated with OATS or ACI.
Surgical Technique:
- Graft is size-matched using imaging (CT/MRI) or templating.
- Defect is debrided to healthy margins.
- Donor graft is harvested, shaped, and press-fit or fixed into the defect site.
- Can be done via mini-open or open approach depending on lesion size.
Advantages:
- Fragment Excision with Curettage:
- Indicated when fragment is unsalvageable
- May require subsequent resurfacing procedure


Leave a Reply