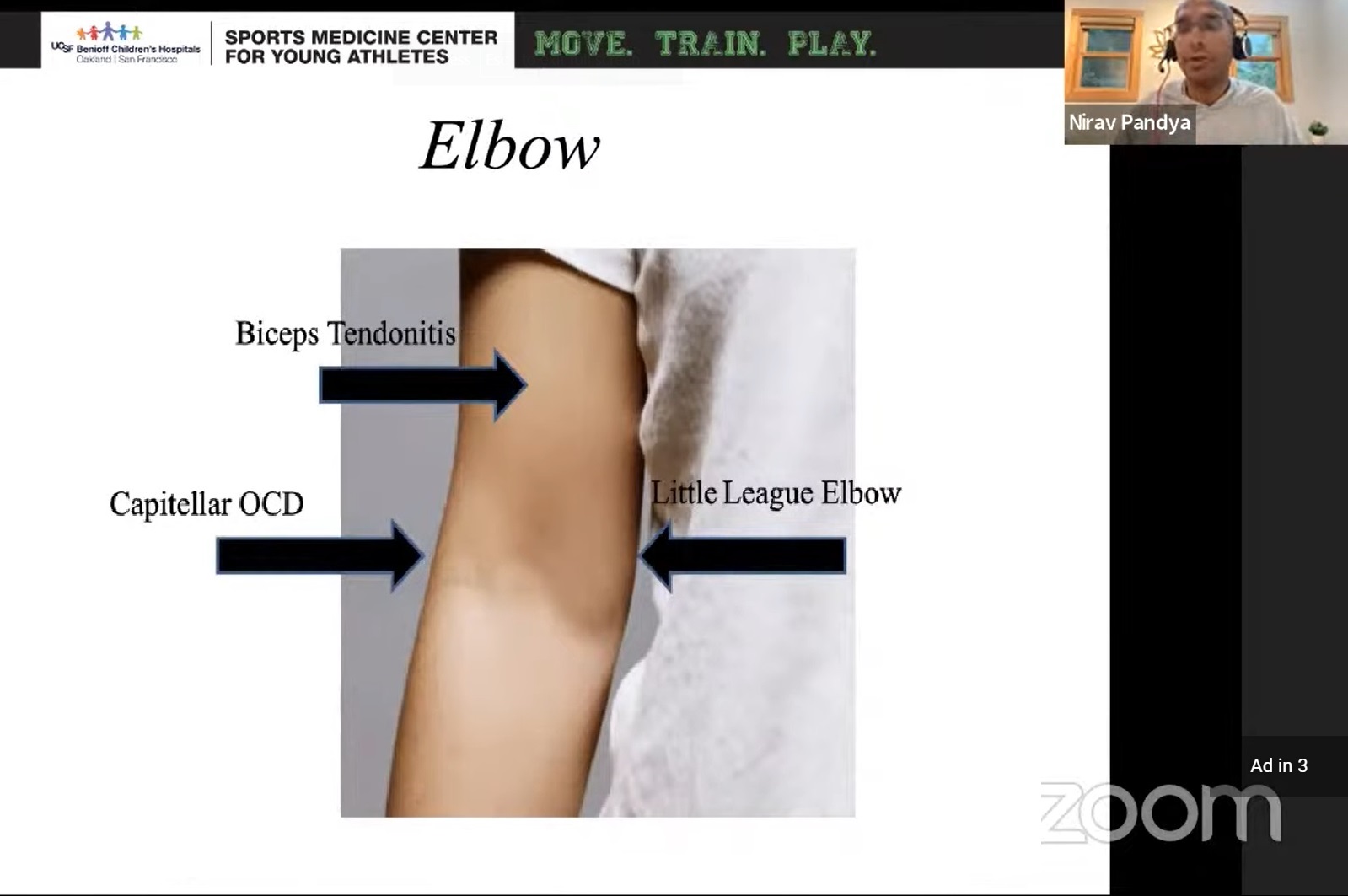
Courtesy: Nirav Pandya MD, Chief of Paediatric Orthopaedics, University of California at San Francico, California, USA
Definition
Osteochondritis Dissecans (OCD) of the capitellum is an injury involving the articular cartilage and subchondral bone of the capitellum.
It is thought to result from:
- Repetitive valgus and compressive loading of the elbow
- Relative vascular insufficiency during skeletal development
- Repetitive microtrauma from sports participation
Why Is It Becoming More Common?
Contributing factors include:
- Early sports specialization
- Year round participation in a single sport
- High training volumes
- Increased competitive pressure
Prevention Rule
Weekly training hours should not exceed the athlete’s age.
Examples:
- 12 year old ? ? 12 hours/week
- 15 year old ? ? 15 hours/week
Encourage participation in multiple sports rather than year round single sport specialization.
Epidemiology
Typical Patient
- Age: 12 to 19 years
- Predominantly males
- Adolescent athletes
High Risk Sports
- Baseball pitchers
- Gymnasts
- Tennis players
- Throwing athletes
Pathophysiology
Repetitive loading causes compression between:
- Capitellum
- Radial head
This leads to:
- Cartilage injury
- Subchondral bone damage
- Fragment instability
- Loose body formation
Clinical Presentation
Symptoms
Lateral Elbow Pain
The hallmark symptom.
Activity Related Pain
- Throwing
- Gymnastics
- Racquet sports
Mechanical Symptoms
- Locking
- Catching
- Clicking
Performance Decline
- Reduced throwing velocity
- Loss of control
- Decreased athletic performance
Important History
Look for:
- Overuse history
- High training volume
- Year round participation
- Pain during sports activity
- Mechanical symptoms
Clinical Examination
Findings
- Tenderness over lateral capitellum
- Reduced elbow range of motion
- Extension loss
- Locking episodes
- Stiffness
Assess the Entire Kinetic Chain
Evaluate:
- Glenohumeral internal rotation
- Shoulder motion
- Core strength
- Lower limb strength
- Throwing mechanics
Differential Diagnosis
Panner Disease vs Capitellar OCD
| Feature | Panner Disease | Capitellar OCD |
|---|---|---|
| Age | 6 to 10 years | 12 to 19 years |
| Pain | Diffuse | Localized lateral pain |
| X ray | Diffuse capitellar involvement | Focal lesion |
| Prognosis | Self limiting | May require surgery |
Key Pearl
Panner disease occurs in younger children and generally heals with observation.
OCD occurs in older adolescents and may progress to instability and loose bodies.
Imaging
Plain Radiographs
May show:
- Capitellar lucency
- Flattening
- Fragmentation
- Loose bodies
MRI (Most Important Investigation)
MRI helps determine:
- Stability of lesion
- Cartilage integrity
- Presence of loose bodies
- Healing potential
MRI Signs of Instability
- Fluid behind the lesion
- Fragmentation
- Cyst formation
- Cartilage disruption
Treatment
Non Operative Treatment
Indications
- Stable lesion
- Small lesion
- Open growth plates
- Intact cartilage
- No fluid behind lesion
Treatment
- Rest
- Activity modification
- Temporary immobilization if required
- Cessation of throwing sports
Outcomes
Best results occur in younger patients with open physes and stable lesions.
Operative Treatment
Indications:
- Unstable lesion
- Loose body formation
- Failed conservative treatment
- Closed growth plates
- Mechanical symptoms
1. Fragment Fixation
Indications
- Early unstable lesions
- Viable osteochondral fragment
- Good cartilage quality
Advantages
- Preserves native cartilage
- Excellent healing when performed early
2. Arthroscopic Debridement and Microfracture
Procedure
- Remove unstable cartilage
- Debride lesion
- Create microfracture holes to stimulate fibrocartilage formation
Results
- Approximately 60% return to sport
- Less predictable in elite athletes
Limitation
Fibrocartilage is biomechanically inferior to native hyaline cartilage.
3. Osteochondral Autograft Transfer (OATS)
Current Gold Standard
Procedure:
- Harvest osteochondral plug from the knee
- Transfer cartilage and subchondral bone to capitellar defect
Advantages
- Restores hyaline cartilage
- Excellent durability
- Highest return to sport rates
Best Candidates
- Competitive athletes
- Large lesions
- Failed previous procedures
4. Osteochondral Allograft
Indications
- Large lesions
- Desire to avoid donor site morbidity
Advantages
- No donor site pain
- Ability to reconstruct large defects
Poor Prognostic Factors
Associated with worse outcomes:
- Older age
- Closed growth plates
- Large lesions
- Unstable lesions
- Cyst formation
- Significant motion loss
- Elite overhead athletes
Causes of Treatment Failure
- Early return to sport
- Persistent overuse
- Poor rehabilitation compliance
- Failure to correct throwing mechanics
- Untreated kinetic chain abnormalities
Management of Failed Cases
Options include:
- Revision OATS procedure
- Osteochondral allograft transplantation
- Correction of biomechanical abnormalities
- Modification of sports participation
In some athletes, changing to a lower stress sport may provide the most reliable long term solution.
Key Clinical Pearls
- Lateral elbow pain in an adolescent athlete should be considered OCD until proven otherwise.
- MRI is the most important investigation for staging and treatment planning.
- Stable lesions in skeletally immature athletes may heal with non operative treatment.
- Microfracture produces fibrocartilage and has limited success in elite athletes.
- OATS currently provides the most predictable return to sport in high demand athletes.
- Prevention through limiting overuse and avoiding early sports specialization remains the best treatment.
Leave a Reply