Courtesy: Dr Bruno Olory MD, Foot and Ankle Surgeon, DOha, Qatar
Osteochondral Lesions of the Talus (OLT): Overview and Management
Introduction
Osteochondral lesions of the talus (OLT) are injuries involving the articular cartilage and subchondral bone of the talar dome.
They are commonly seen following:
- Ankle sprains
- Ankle fractures
These lesions are an important cause of persistent ankle pain and dysfunction
Epidemiology
Incidence
- Approximately 27 cases per 100,000 persons/year
Association with Other Injuries
-
70% of ankle fractures
-
50% of ankle sprains with instability
Demographics
- Mean age: ~31 years
- Male predominance (~63%)
- Right ankle more commonly affected
Relevant Anatomy
Tibiotalar Joint Characteristics
- Highly congruent joint
- Uneven cartilage distribution
Cartilage Thickness
- Tibial cartilage: relatively uniform
- Talar cartilage:
- Thicker anteriorly
- Thinner posteriorly
Pathophysiology
Effect of Injury
Ankle instability or fracture leads to:
- Altered joint congruency
- Abnormal load distribution
Role of Synovial Fluid
When cartilage is damaged:
- Synovial fluid enters subchondral bone
Results
- Subchondral sclerosis
- Osteolysis
- Cyst formation
Progressive cartilage deterioration
Distribution of Lesions
Common Locations
- Medial talar dome: ~60%
- Central lesions: >80%
Association
- Anterolateral lesions strongly linked to instability (~93%)
Lesion Characteristics
Medial Lesions
- Larger
- Deeper
Lateral Lesions
- More superficial
- Often traumatic
Rare Lesions
- Tibial plafond: ~2.6%
- Bipolar lesions: <1%
OLT in Athletes
- ~42% prevalence on MRI in professional athletes
- Strong association with:
- Repetitive trauma
- Ankle sprains
Mechanism of Injury
Acute
- Forced inversion injury
Chronic
- Repeated ankle sprains
- Progressive cartilage damage
Osteochondritis Dissecans (OCD) of the Talus
Definition
A subtype of OLT, typically seen in:
- Children and adolescents
- Mean age: ~11 years
Etiology
- Microtrauma (most accepted)
- Vascular insufficiency
- Degenerative changes
Clinical Presentation
Symptoms
- Ankle pain during weight-bearing
- Pain after sports
- Swelling
- Stiffness
Mechanical Symptoms
- Clicking — cartilage flap
- Locking — loose body
- Instability sensation
Classification Systems
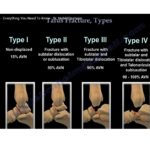
1. Berndt and Harty Classification (X-ray Based)
| Stage | Description |
|---|---|
| I | Subchondral compression |
| II | Partially detached fragment |
| III | Completely detached fragment |
| IV | Displaced fragment |
Limitation
- Up to 40% not visible on X-ray
2. Loomer Classification
- Adds Stage V:
- Subchondral cyst
3. MRI Classification
- Assesses:
- Cartilage integrity
- Bone edema
- Stability
4. Arthroscopic Classification (ICRS)
| Grade | Description |
|---|---|
| I | Soft cartilage |
| II | Partial defect |
| III | Deep defect |
| IV | Exposed bone |
Non-Operative Management
Goals
- Pain relief
- Functional restoration
Treatment Options
- Immobilization (4–6 weeks)
- Non-weight bearing
- Physiotherapy
- Orthotics
- Weight reduction
- NSAIDs
Indications
- Stage I
- Stage II
- Small Stage III lesions
Outcomes
- ~86% pain-free at 2 years
Limitation
-
50% may develop osteoarthritis long-term
Biological Therapies
Options
- Platelet-rich plasma (PRP)
- Bone marrow aspirate concentrate (BMAC)
Role
- Pain reduction
- Functional improvement
Evidence
- Currently inconclusive
Surgical Management
Key Determinants
- Lesion size
- Depth
- Stability
1. Debridement and Excision
Indication
- Small unstable fragments
Outcome
- ~50–77% success
2. Fragment Fixation
Indications
- Large acute fragment
- Good bone stock
Technique
- Reduction
- Subchondral drilling
- Fixation with:
- Headless screws
- Bioabsorbable pins
Criteria
- Size >100 mm²
- Depth >5 mm
Outcome
- ~89% success
3. Drilling Techniques
Indication
- Intact cartilage
Goal
- Stimulate revascularization
Outcome
- ~85% success
4. Microfracture (Gold Standard for Small Lesions)
Indications
- <150 mm²
- Depth <5 mm
- ICRS Grade III
Mechanism
- Bone marrow stimulation
- Fibrocartilage formation
Outcome
- ~80% good results
5. Autologous Chondrocyte Implantation (ACI)
Technique
- Two-stage procedure:
- Cartilage biopsy
- Cell culture
- Reimplantation
Outcome
- ~80% success
6. MACI (Matrix-Induced ACI)
Advantages
- Scaffold-based
- Easier implantation
- Similar outcomes to ACI
7. Minced Cartilage Technique
Procedure
- Harvest cartilage
- Mince and mix with PRP/BMAC
- Implant into defect
Outcome
- ~78% success
8. Osteochondral Autograft Transfer (OATS)
Indications
- Large lesions
- Deep lesions
- Subchondral cysts
Technique
- Cartilage plugs harvested from knee
- Transferred to talus
Outcome
-
85% success
Surgical Exposure
Challenge
- Most lesions are medial and central
Solution
Medial Malleolar Osteotomy
- Provides direct access
Fixation
- Screws or plate fixation
- Minimum three screws recommended
Key Treatment Principles
Treat Only Symptomatic Lesions
- Incidental lesions — no surgery
Based on Lesion Size
Small Lesions
- <100 mm²
- <5 mm depth
Treatment
- Microfracture
- Biological repair techniques
Large Lesions
-
100 mm²
-
5 mm depth
Treatment
- Osteochondral grafting (OATS)
Address Associated Pathology
- Ankle instability
- Malalignment
- Loose bodies
Failure to address leads to poor outcomes
Key Takeaways
- OLT commonly follows ankle trauma
- MRI is essential for diagnosis
- Treatment depends on:
- Size
- Depth
- Stability
Management Summary
- Small lesions — microfracture or biological repair
- Large lesions — osteochondral grafting
- Always treat associated instability
Clinical Insight
Successful outcomes depend on:
- Accurate diagnosis
- Appropriate procedure selection
- Correction of associated pathology
Leave a Reply