Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Cervical Disc Herniation and Radiculopathy
Introduction
Cervical disc herniation occurs when disc material compresses a cervical nerve root, producing radiculopathy.
Typical manifestations include:
- Neck pain
- Radiating arm pain
- Sensory symptoms
- Weakness
- Reflex abnormalities
Common Levels
The most commonly affected levels are:
- C6–C7
- C5–C6
These account for the majority of cervical radiculopathies.
Pathophysiology
Disc herniation leads to:
- Compression and inflammation of cervical nerve roots
This produces:
- Pain
- Sensory disturbance
- Motor weakness
- Reflex changes
Clinical Features
Pain
Typical pain pattern includes:
- Neck pain radiating into the ipsilateral upper limb
- Dermatomal distribution of symptoms
Associated Symptoms
Patients may complain of:
- Numbness
- Paresthesia
- Weakness
Aggravating Factors
Symptoms may worsen with:
- Coughing
- Sneezing
- Neck movement
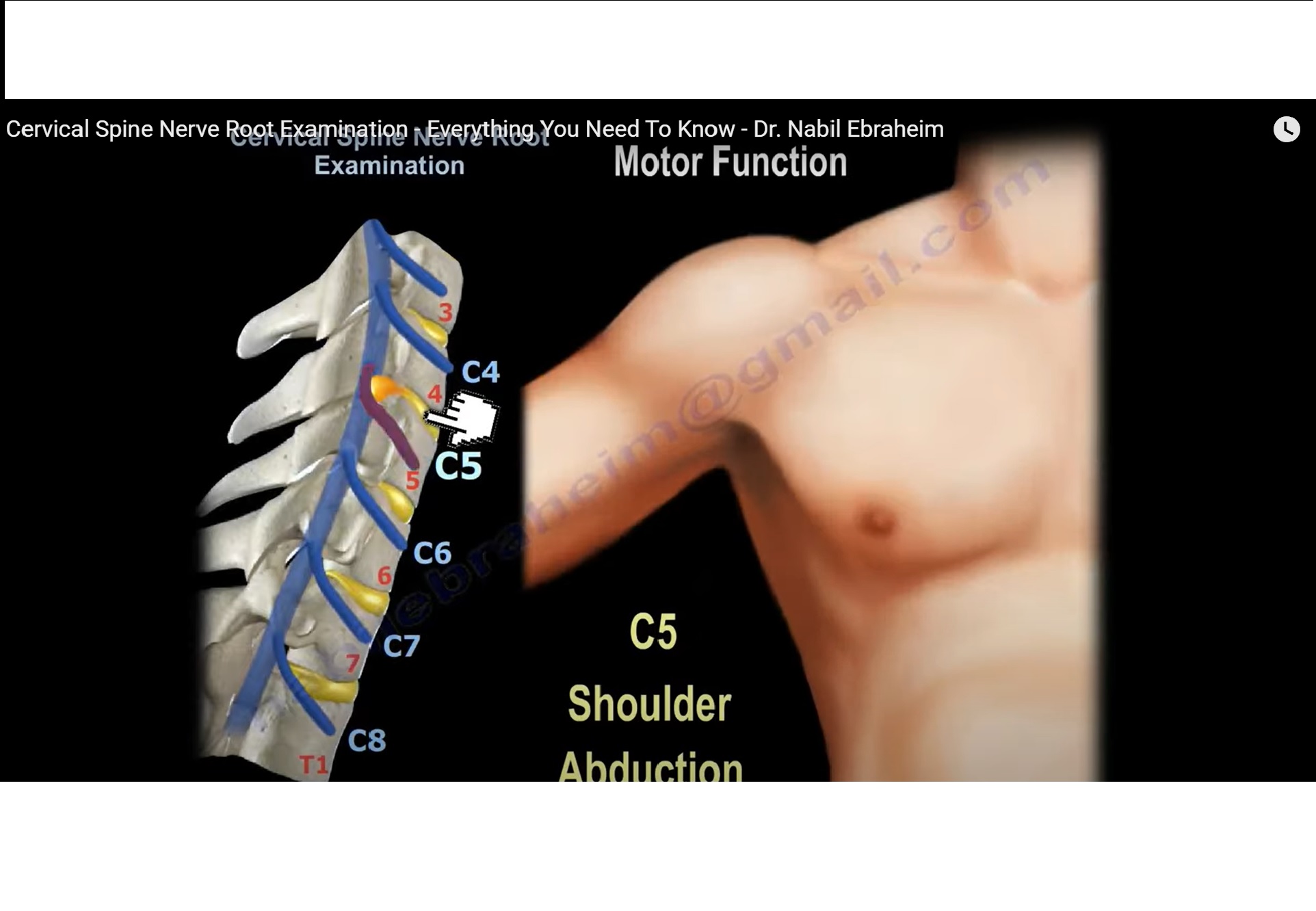
Clinical Examination
Each cervical nerve root should be evaluated for:
- Motor function
- Reflex changes
- Sensory deficit
A systematic examination is essential.
Root-wise Clinical Findings
| Disc Level | Root Affected | Motor Deficit | Reflex Change | Sensory Distribution |
|---|---|---|---|---|
| C3–C4 | C4 | Diaphragm (phrenic nerve) | None | Shoulder region |
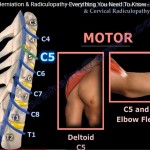
| C4–C5 | C5 | Deltoid, elbow flexion | Reduced biceps reflex | Lateral shoulder |
| C5–C6 | C6 | Wrist extension, elbow flexion | Reduced brachioradialis reflex | Thumb and index finger |
| C6–C7 | C7 | Triceps, wrist flexion, finger extension | Reduced triceps reflex | Middle finger |
| C7–T1 | C8 | Finger flexion | No reliable reflex | Medial two fingers |
| T1–T2 | T1 | Interossei muscles | No reliable reflex | Medial forearm |
Important Clinical Correlations
C4 Root
- Contributes to the phrenic nerve
- Severe involvement may affect diaphragmatic function and respiration
C5 Root
Features include:
- Weak shoulder abduction
- Reduced biceps reflex
C6 Root
Typical findings:
- Weak wrist extension
- Sensory loss involving thumb and index finger
C7 Root
Most common cervical radiculopathy.
Features include:
- Weak triceps
- Reduced triceps reflex
- Middle finger numbness
C8 Root
Findings include:
- Weak finger flexion
- Reduced grip strength
- No dependable reflex
T1 Root
Involvement produces:
- Weak finger abduction and adduction
- Interossei weakness
Important Examination Principles
Always correlate:
- Motor weakness
- Reflex changes
- Sensory loss
Dermatomal distribution is a key diagnostic clue.
Important Cervical Spine Rule
In the cervical spine:
- Disc herniation usually affects the lower nerve root
Example:
- C6–C7 disc herniation affects the C7 root
This is called the:
- Lower root rule
Management
Conservative Treatment
First-line treatment includes:
- NSAIDs
- Physiotherapy
- Activity modification
Most patients improve without surgery.
Indications for Surgery
Surgery may be indicated for:
- Persistent symptoms beyond 6–12 weeks
- Progressive neurological deficit
- Significant weakness
- Myelopathy
High-Yield Clinical Pearls
- Most common cervical disc level: C6–C7
- Most common radiculopathy: C7
- Middle finger numbness suggests C7 involvement
- Thumb and index finger symptoms suggest C6 involvement
- Biceps reflex corresponds mainly to C5
- Triceps reflex corresponds mainly to C7
- There is no reliable reflex for C8 radiculopathy
Related Posts
 Neck pain, Cervical Disc Herniation and Radiculopathy
Neck pain, Cervical Disc Herniation and RadiculopathyCourtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
 Cervical Disc Herniation and Radiculopathy
Cervical Disc Herniation and RadiculopathyCourtesy: Prof Nabil Ebrhaeim, University of Toledo, Ohio, USA
- Cervical Disc Herniation
Courtesy: Prof Nabile Ebraheim, University of Toledo, Ohio, USA
Leave a Reply