This exam must be completed in 20 minutes. Click here to start the exam
Courtesy: Zaid Al-RUb, FRCS Orth, Founder, OrthoPass
Courtesy: Zaid Al-Rub, Founder and CEO, OrthoPass
- Gap Balancing in Total Knee Replacement
Scenario
- Primary Total Knee Replacement (TKR).
- After distal femur and proximal tibial cuts:
- Extension gap – tight
- Flexion gap – balanced
First Step
Posterior capsule release
Principles of Gap Balancing
- Rule 1: Address soft tissue before additional bone resection.
- Rule 2:
- Distal femur cut ? affects extension gap
- Rule 3:
- Posterior femoral condyles ? affect flexion gap
- Rule 4:
- Proximal tibia ? affects both flexion and extension
Practical Approach
- Tight in extension only:
- Posterior capsule release
- If unresolved ? resect more distal femur
Ideal Gap Shape
- Balanced knee ? rectangular flexion and extension gaps
Unbalanced Knee
- Trapezoidal gap
- Often occurs in varus knees with tight medial structures
- Total Knee Replacement in Valgus Deformity
Epidemiology
- Valgus knees represent ~10% of TKR cases
Pathology
- Medial Collateral Ligament (MCL) ? stretched or incompetent
- Lateral structures ? contracted
Surgical Goal
Release tight lateral structures to restore balance.
Important Surgical Principles
- Perform releases with knee in extension
- Check balance after each release
- Perform minimal necessary releases
Structures Often Released
Common sequence (varies between surgeons):
- Osteophytes
- Lateral capsule
- Iliotibial band
- Popliteus tendon
- Lateral collateral ligament (last resort)
Correct MCQ Concept
- Valgus deformity >15° often requires release of:
- Iliotibial band
- Popliteus tendon
Complication
- Risk of common peroneal nerve traction injury
- Total Hip Replacement vs Hemiarthroplasty in Neck of Femur Fracture
Total Hip Replacement (THR)
Advantages
- Better:
- Function
- Quality of life
- Patient satisfaction
Disadvantages
- Longer surgery
- Higher dislocation rate
- Higher revision rate in some observational studies
Hemiarthroplasty
Advantages
- Shorter surgery
- Lower dislocation risk
Disadvantages
- Acetabular cartilage wear
- Worse functional outcome
Key MCQ Point
Compared with hemiarthroplasty, THR shows:
Higher revision rate
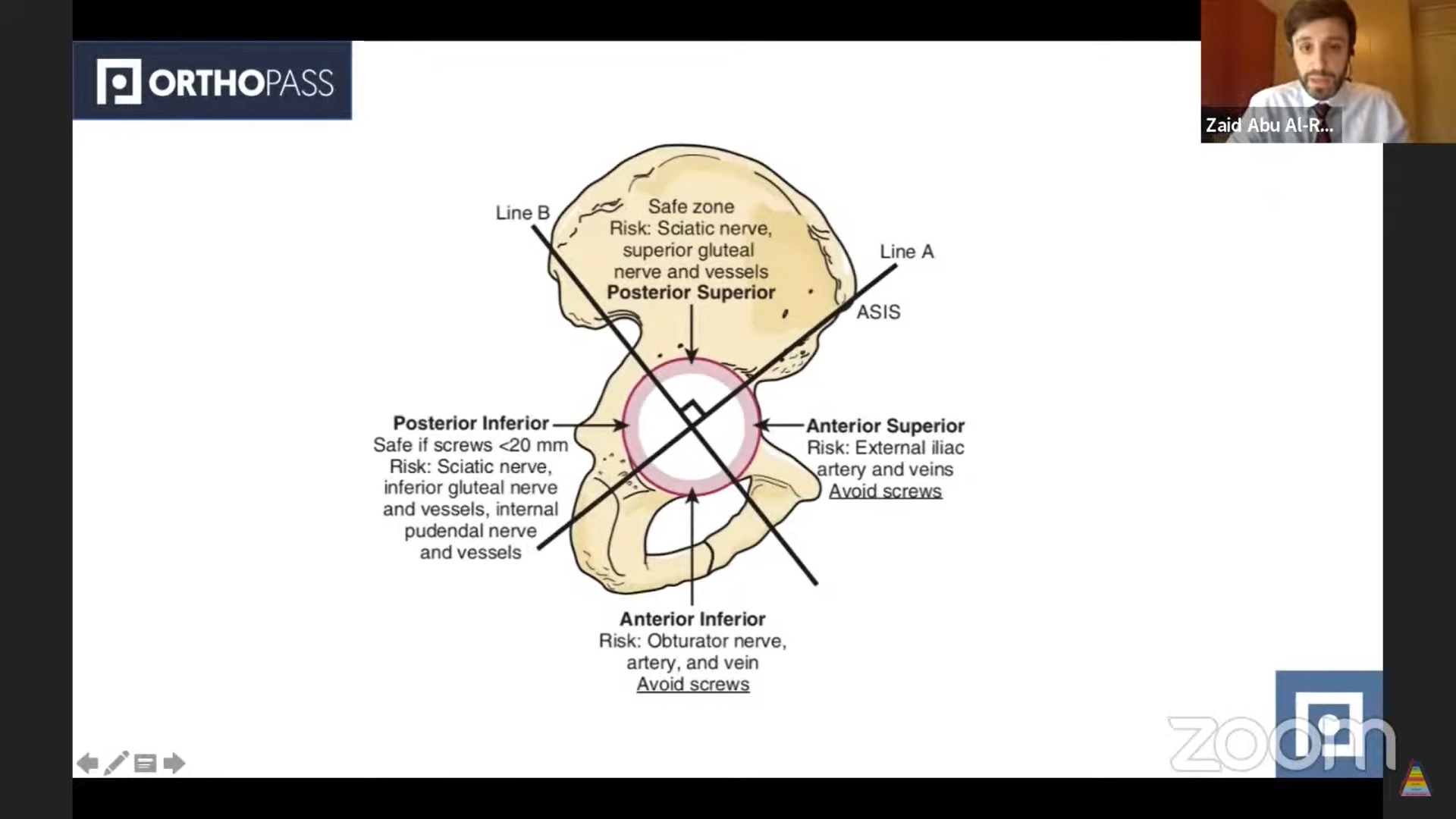
- Safe Zone for Acetabular Screw Placement
During Total Hip Replacement, acetabular screws should be placed in the:
Posterosuperior quadrant
Acetabular Quadrants
Defined by two lines from the center of the acetabulum to:
- Anterior Superior Iliac Spine (ASIS)
- Posterior Superior Iliac Spine (PSIS)
Safe Zone
- Posterosuperior quadrant
Reason
Avoids injury to:
- External iliac vessels
- Obturator vessels
- Sciatic nerve
- Erb’s Palsy (Obstetric Brachial Plexus Injury)
Nerve Roots
- C5–C6
Typical Limb Position (Waiter’s Tip)
- Shoulder adduction
- Shoulder internal rotation
- Elbow extension
- Forearm pronation
- Wrist flexion
Muscles Affected
- Deltoid
- Supraspinatus
- Infraspinatus
- Biceps
Characteristic Complication
- Posterior shoulder dislocation or subluxation
MCQ Key Point
Anterior shoulder dislocation is NOT typical
- Developmental Dysplasia of the Hip (DDH)
Age in Question
6 months
Most Sensitive Clinical Sign
Limited hip abduction in flexion
Test Usefulness by Age
| Test | Age group |
| Ortolani test | Neonates |
| Barlow test | Neonates |
| Galeazzi test | Later infancy |
| Limited abduction | >3–6 months |
Asymmetric Skin Folds
- Low diagnostic value
- High false positive rate
- Indications for Surgery in Thoracolumbar Burst Fracture
Common criteria for surgery include:
- Kyphosis >30°
- Vertebral body height loss >50%
- Canal compromise >50%
- Progressive neurological deficit
Important MCQ Concept
- Canal compromise alone is NOT an indication
Definition of Burst Fracture
- Failure of:
- Anterior column
- Posterior vertebral body cortex
- With retropulsion of fragments
- Adolescent Idiopathic Scoliosis Management
Case Parameters
- Age: 12 years
- Cobb angle: 30°
- Risser grade: 2
Management
Brace treatment
General Treatment Guidelines
| Cobb Angle | Management |
| <20° | Observation |
| 20–40° | Bracing |
| >45° | Surgery |
Risser Grade Meaning
- Indicates skeletal maturity
- 0–1 ? rapid growth phase
- 4–5 ? skeletal maturity
- Structure of Articular Cartilage
Layers of cartilage:
- Superficial zone
- Middle zone
- Deep zone
- Tidemark
- Calcified cartilage
Proteoglycan Distribution
- Highest concentration ? Deep zone
Collagen Orientation
| Layer | Fibre orientation |
| Superficial | Parallel |
| Middle | Oblique |
| Deep | Perpendicular |
Function
- Superficial ? shear resistance
- Deep ? compressive load resistance
- Principles of Plate Fixation
Correct Principle
Maximum plate efficiency occurs when applied to the tension side of the bone
Additional Biomechanics Facts
Pullout strength depends on:
- Thread diameter
Plate bending rigidity:
- Proportional to thickness³
Material properties
- Stainless steel modulus > titanium
Application
- Tension band principle in fracture fixation
Major References Verified
- Campbell’s Operative Orthopaedics
- Rockwood and Green’s Fractures in Adults
- Lovell and Winter’s Pediatric Orthopaedics


Leave a Reply