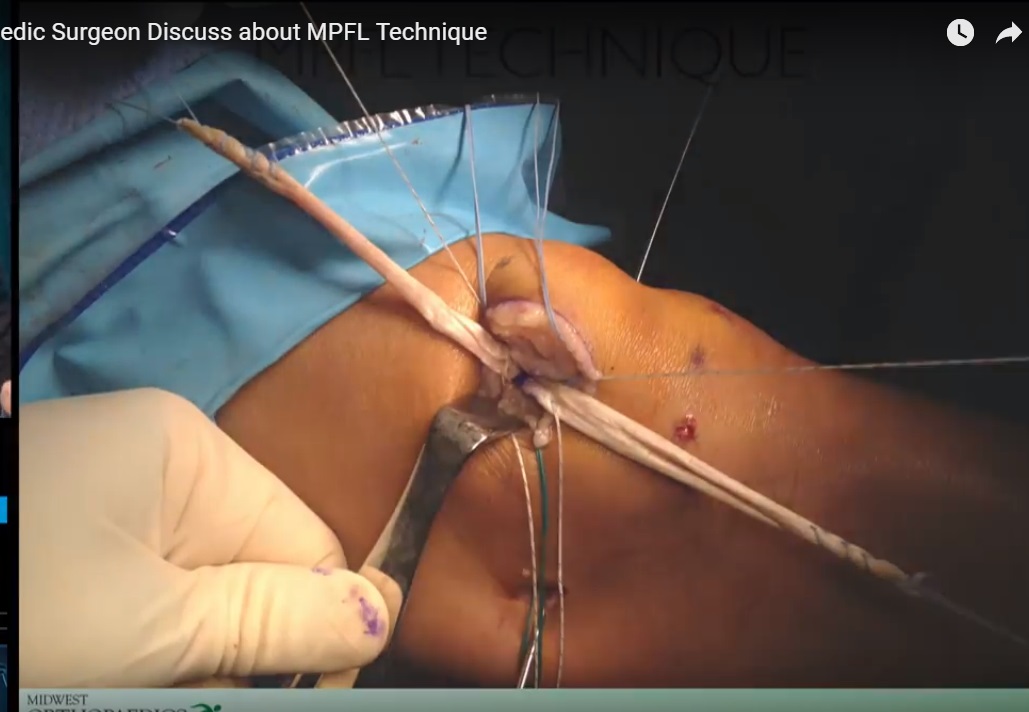
Courtesy: Dr B Sabnis, Ashok Shyam TV, Ortho
MPFL Anatomy Overview
-
The medial patellofemoral ligament (MPFL) is a fan-shaped structure.
-
Length varies with body habitus:
-
Approximately 46–49 mm in smaller Asian populations.
-
Approximately 50–56 mm in Caucasian populations.
-
Indian population typically in between.
-
-
Width ranges widely (3–30 mm), consistent with its fan-shaped configuration.
Patellar Attachment
-
Located on the proximal half of the patella.
-
Rarely extends beyond the equator.
-
Positioned more toward the dorsal aspect of the medial patella.
-
Lies between layer II and layer III.
Femoral Attachment
-
Not a single point.
-
More accurately described as a “cloud” of attachment.
-
Located between:
-
Medial epicondyle
-
Adductor tubercle
-
Anatomic landmarks are generally reliable but vary in dysplastic knees.
Anatomy vs Isometry: The Core Debate
Important Principle
The MPFL is a non-isometric ligament.
-
Its length changes during knee motion.
-
Therefore, it cannot behave like a perfectly isometric structure.
-
The knee is not a simple hinge of two perfect circles.
Definition of Isometry
-
A truly isometric ligament would not change length through flexion-extension.
-
The MPFL does change length.
-
Therefore, strict isometric reconstruction is not anatomically correct.
Radiographic Landmarks and Schöttle’s Point
-
Schöttle’s point is widely described for femoral tunnel placement.
-
However:
-
Radiographic landmarks are not perfectly reproducible.
-
Trochlear dysplasia alters anatomy.
-
Fluoroscopy alone may not guarantee accuracy.
-
-
Studies show variability in tunnel placement even among expert surgeons.
Conclusion:
Radiographic landmarks should guide but not dictate tunnel placement.
Anatomic Reconstruction Approach
Surgical Steps (Anatomic Philosophy)
-
Identify proximal patellar border.
-
Create medial patellar trough.
-
Insert two anchors in proximal half of patella.
-
Identify femoral landmarks:
-
Medial epicondyle
-
Adductor tubercle
-
Approximately 1 cm posterior to medial epicondyle (flexed knee view)
-
Approximately 5 mm anterior and distal to adductor tubercle
-
-
Pass graft between layer II and layer III.
-
Fix femoral side after confirming position.
Short-term results:
-
Good stability.
-
Low early failure rates.
-
Long-term data still evolving.
Counterpoint: Functional Isometry Matters
Although MPFL is non-isometric:
-
It should behave nearly isometric between 0° and 60° of flexion.
-
It should loosen beyond 60–90° of flexion.
-
It must never tighten in deep flexion.
Why This Matters
Improper femoral tunnel placement can cause:
-
Overconstraint.
-
Increased patellofemoral contact pressure.
-
Pain.
-
Cartilage damage.
-
Graft failure.
Most MPFL failures are due to incorrect femoral tunnel placement.
Practical Approach: Blended Strategy
Stepwise Method
-
Palpate anatomic landmarks.
-
Insert guide pin.
-
Check graft behavior through range of motion.
-
Confirm with fluoroscopy if needed.
Isometric Check Technique
-
Mark graft at two points.
-
Flex knee from 0° to 90°.
-
Desired behavior:
-
Minimal length change from 0°–60°.
-
Slight loosening beyond 60°.
-
Never tightening in flexion.
-
Challenges in Abnormal Anatomy
In patients with:
-
Trochlear dysplasia
-
Patella alta
-
Severe maltracking
-
Significant tibial tubercle lateralization
Anatomic landmarks may not correspond to ideal functional positioning.
In these cases:
-
Isometric behavior check becomes critical.
-
Purely fluoroscopic placement may be unreliable.
Pediatric Considerations
-
Open distal femoral physis must be protected.
-
Avoid physeal violation.
-
Options:
-
Distal and anterior angulation of tunnel.
-
Soft tissue techniques.
-
Adductor sling techniques.
-
-
Anatomic location may need modification to preserve physis.
Important:
Some skeletally immature patients with severe deformity may require staged procedures once skeletal maturity is reached.
MQTFL vs MPFL Discussion
-
Medial quadriceps tendon femoral ligament (MQTFL) avoids patellar drilling.
-
Reduces risk of patellar fracture.
-
Some surgeons have transitioned entirely to this technique.
-
Avoid overtensioning in all techniques.
Key Shared Principles
Both perspectives agree on critical points:
-
Avoid overtightening.
-
Avoid overconstraint.
-
Confirm graft behavior dynamically.
-
Do not rely solely on fluoroscopy.
-
Do not rely solely on palpation.
-
Individualize based on patient anatomy.
When to Be Especially Careful
-
Severe trochlear dysplasia.
-
Significant patella alta.
-
Large J-sign.
-
Pediatric open physis.
-
Complex deformity where osteotomy may eventually be required.
Take-Home Messages
-
MPFL is anatomically well described but functionally complex.
-
It is non-isometric by nature.
-
Femoral tunnel malposition is the most common cause of failure.
-
Functional behavior through early flexion arc is critical.
-
Anatomy should guide placement.
-
Isometric testing should validate placement.
-
Avoid overtightening at all costs.
-
Pediatric patients require additional caution regarding physeal safety.
Conclusion
The debate is not anatomy versus isometry.
The correct approach is:
-
Anatomic landmark identification
-
Followed by functional isometric validation
-
With fluoroscopic confirmation when necessary
Successful MPFL reconstruction depends less on philosophy and more on precise femoral positioning and avoidance of overconstraint.


Leave a Reply