Courtesy: Dr Jordi Sanchez Ballester, FRCS Orth, Liverpool, UK
Initial Clinical Assessment
History and Examination
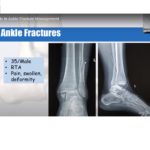
A thorough history and clinical examination are essential in evaluating ankle injuries.
Typical Presentation
-
Painful, swollen ankle
-
History of inversion or eversion injury
Differential Diagnosis
When assessing ankle trauma, always consider:
-
Ligament injuries
-
Tendon injuries
-
Osteochondral lesions
-
Syndesmotic injuries
-
Fractures of the ankle and foot
Clinical Tip:
Avoid focusing solely on fractures—associated soft tissue injuries are commonly missed.
Ottawa Ankle Rules
Purpose
Used in emergency settings to determine the need for radiographs, thereby:
-
Reducing unnecessary imaging
-
Improving efficiency
Indications for Ankle X-ray
An X-ray is indicated if there is pain in the malleolar zone along with:
-
Bone tenderness at:
-
Posterior edge/tip of lateral malleolus
-
Posterior edge/tip of medial malleolus
-
-
Inability to bear weight for 4 steps
Key Questions in Ankle Fracture Evaluation
Once a fracture is identified, two critical questions guide management:
-
Is the fracture displaced or undisplaced?
-
Is the fracture stable or unstable?
Undisplaced Ankle Fractures
Epidemiology
-
Approximately 75% of ankle fractures are undisplaced
Definition
-
Talar alignment is maintained within the ankle mortise
-
Minor fibular rotation may be present, but mortise remains congruent
Key Indicator: Talar Shift
Significance
-
Indicates instability and displacement
Radiographic Criteria
-
Medial clear space > 4 mm
OR -
Medial clear space > 2 mm more than superior clear space
Presence of talar shift = Displaced & unstable fracture
Stability of Ankle Fractures
Stable Fractures
Typically include:
-
Weber A or Weber B fractures
-
No medial tenderness
-
No medial swelling or bruising
-
Usually low-energy injuries
Medial Tenderness: Does It Always Mean Instability?
Not necessarily.
Explanation
-
Injury may involve only the superficial deltoid ligament
-
The deep deltoid ligament may remain intact
-
If deep deltoid ligament is intact – ankle remains stable
Biomechanics of Ankle Stability
Role of Deep Deltoid Ligament
-
Primary stabilizer of the ankle mortise
-
Prevents lateral talar shift
If Intact
-
Talus remains centered
-
Fracture may still be stable
If Ruptured
-
Talus shifts laterally
-
Leads to unstable fracture
Role of Weight-Bearing Radiographs
If Deltoid Ligament Intact
-
Weight-bearing tightens ligament
-
Mortise remains congruent
If Ruptured
-
Weight-bearing reveals talar shift
-
Confirms instability
Fibular Rotation: Important Clarification
-
Apparent external rotation on X-ray is often due to:
-
Internal rotation of proximal fibula
-
If mortise is congruent ? fracture is still undisplaced
-
Management of Undisplaced Stable Fractures
Example
-
Lateral malleolus fracture without medial tenderness
Treatment
-
Functional management
-
Pain control
-
External support
Options
-
Ankle brace
-
Stirrup splint
-
Tubigrip
Weight Bearing
-
Full weight bearing allowed
Healing & Follow-Up
-
Healing time: ~6 weeks
-
Routine follow-up often not required
-
Excellent union rates
Undisplaced but Potentially Unstable Fractures
Example
-
Lateral malleolus fracture with medial tenderness
Concern
-
Possible deep deltoid ligament injury
Investigation
-
Perform weight-bearing ankle X-ray
Interpretation
Stable
-
Mortise congruent
-
Deep deltoid intact
Unstable
-
Talar shift present
-
Deltoid ligament disrupted
Management
Stable on Weight-Bearing
-
Below-knee cast or walking boot
-
Weight bearing as tolerated
-
Healing: 5–6 weeks
If Displacement Develops
-
Indicates instability
-
Treatment: Open Reduction and Internal Fixation (ORIF)
Management of Displaced / Unstable Fractures
General Principle
-
Most unstable fractures require surgical fixation
Factors Influencing Decision
-
Skin condition
-
Swelling and blisters
-
Patient age
-
Comorbidities
-
Functional demands
Timing of Surgery
-
Immediate (Day 1)
OR -
Delayed until swelling subsides
Indicator
-
Wrinkle sign suggests readiness for surgery
Surgical Fixation Techniques
Lateral Malleolus
Standard Fixation
-
One-third tubular plate
-
Often combined with lag screw
In Osteoporotic Bone
-
Locking anatomical plate preferred
Medial Malleolus
Key Points
-
Usually associated with other fractures
-
Isolated fractures are rare
-
Always rule out Maisonneuve fracture
Standard Fixation
-
Two partially threaded cancellous screws
-
Often with washers
Exceptions
-
Small avulsion fractures may not need fixation
Vertical Fractures
Problem
-
Screw fixation may cause shear displacement
Preferred Treatment
-
Buttress plate fixation
Syndesmotic Injuries
Common In
-
Weber C fractures
-
Always considered unstable
Fixation Options
-
Syndesmotic screw (1.5 cm above joint)
-
One or two screws
-
Weight Bearing
-
Usually non-weight bearing for ~8 weeks
Screw Removal
-
Controversial:
-
Remove at ~12 weeks
-
Or leave in situ
-
Broken screws are usually asymptomatic
-
Tightrope Fixation
Advantages
-
Allows physiological micromotion
-
No need for removal
-
Both screw and tightrope techniques are acceptable
Posterior Malleolus Fracture
Traditional Teaching
-
Fix if >25% articular involvement
Current Concept
-
Fragment size is less important
Key Factor
-
Syndesmotic stability
Importance
-
Attachment site of posterior inferior tibiofibular ligament
Displacement leads to:
-
Syndesmotic instability
-
Increased risk of post-traumatic arthritis
Indications for Fixation
-
Displacement >2 mm
-
Syndesmotic instability
-
Associated complex fractures
Preferred Approach
-
Posterolateral approach
Advantages
-
Direct visualization
-
Improved reduction
-
Allows buttress plating
Mason Classification (Posterior Malleolus)
Type 1
-
Small fragment
-
Treatment: Fibular fixation + syndesmotic stabilization
Type 2A
-
Posterolateral fragment
-
Treatment: Posterolateral plating
Type 2B
-
Posterolateral + posteromedial fragments
-
Treatment: Combined fixation
Type 3
-
Large fragment (pilon-like)
-
Treatment: Posteromedial approach
Evidence-Based Insight
-
Fixation improves:
-
Functional outcomes
-
Syndesmotic stability
-
Slight increase in implant removal rates
-
Special Situations
Ankle Fractures in Diabetic Patients
Key Concern
-
Peripheral neuropathy
Risks
-
Fixation failure
-
Charcot arthropathy
Surgical Considerations
-
Stronger fixation
-
Locking plates
-
Additional syndesmotic screws
Postoperative Care
-
Prolonged non-weight bearing
-
Typically 2–3× longer than non-diabetic patients
Deltoid Ligament Repair
Usually Not Required
Indications
-
Persistent talar displacement after fixation
-
Interposed ligament blocking reduction
-
Significant medial instability
Technique
-
Repair using suture anchors
Hindfoot Nail in Elderly
Indication
-
Frail or very elderly patients
Advantages
-
Early weight bearing
-
Avoids repeated surgeries
Alternative Technique
Percutaneous Steinmann Pin Fixation
-
Inserted from tibia ? talus ? calcaneus
-
Removed after ~12 weeks
Benefits
-
Cost-effective
-
Technically simple
Key Takeaways
-
Always assess stability and displacement
-
Talar shift = instability
-
Weight-bearing X-rays are crucial
-
Most unstable fractures require ORIF
-
Posterior malleolus fixation depends on stability, not size
-
Special populations (e.g., diabetics, elderly) require modified strategies

Leave a Reply