Courtesy: Dr. Hariharan Kartik, Dr Ashok Shyam, Ortho TV
Minimally Invasive Surgery (MIS) for Foot and Ankle Deformity Correction
Background
Traditional open surgical techniques for foot and ankle deformity correction often require extensile exposures, which may result in:
- Significant soft tissue disruption
- Vascular compromise
- Increased wound complications:
- Wound dehiscence
- Infection (sepsis)
These issues are particularly relevant in hindfoot surgery
Philosophy of Minimally Invasive Surgery
Core Principles
Minimally invasive surgery (MIS) aims to:
- Reduce surgical trauma
- Preserve soft tissue circulation
- Decrease postoperative complications
Conceptual Basis
The philosophy parallels arthroscopy, where:
- Smaller incisions
- Less tissue disruption
- Faster recovery
are consistently observed.
Modern Evolution
Advances in:
- Instrumentation
- Imaging (fluoroscopy)
have enabled surgeons to combine traditional surgical principles with minimally invasive techniques.
Instruments and Surgical Technique
Traditional Osteotomy (Open Surgery)
Technique
- Uses oscillating saws for linear bone cuts
Advantages
- Direct visualization
- Minimal bone loss
Limitations
- Larger incisions
- Greater soft tissue disruption
Burr-Based MIS Osteotomy
Technique
- Uses rotational burrs (2–3 mm diameter)
- Creates controlled bone cuts through small incisions
Key Features
- Performed via stab incisions
- Produces minimal bone debris
- Requires fluoroscopic guidance (mini C-arm)
Advantages
- Minimal soft tissue damage
- Indirect bone cutting
- Improved cosmetic outcome
Technical Note
- “Pencil grip” technique provides tactile feedback
- Requires dedicated MIS instruments
MIS Procedures in the Forefoot
1. Minimally Invasive Dorsal Cheilectomy
Indication
- Hallux rigidus
Technique
- ~3 mm stab incision
- Burr removal of dorsal osteophytes
Advantages
- Performed under regional anesthesia
- No sutures often required
- Early mobilization
Clinical Benefit
- Return to activity (including tiptoe walking) within ~1 week
- Particularly useful in athletes
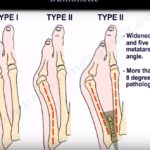
2. Minimally Invasive Hallux Valgus Correction
Principles
- Lateral soft tissue release
- Distal metatarsal osteotomy (Chevron-type)
Technical Considerations
- Burr osteotomy may cause bone loss
- Compensation strategies:
- Angulated osteotomy
- Distal translation of metatarsal head
Additional Procedure
- Akin osteotomy for proximal phalanx deformity
Indications
- Initially mild–moderate deformity
- Now expanding to severe deformities
3. MIS for Metatarsalgia
Traditional Issues
- Weil/Helal osteotomies may cause:
- Floating toe deformity
MIS Technique
- Multiple metatarsal osteotomies via small portals
Advantages
- Preserves collateral ligaments
- Maintains natural metatarsal parabola
- Reduces floating toe incidence
Postoperative Care
- Early weight-bearing from day 1
4. Tailor’s Bunion (Bunionette) Correction
Technique
- Minimally invasive osteotomy of fifth metatarsal
Mechanism
- Correction aided by soft tissue forces
- Interosseous muscle pull assists alignment
MIS in Hindfoot Osteotomies
Concept
- Multiplanar correction through 3–4 mm portals
Types of Corrections
- Sagittal plane
- Coronal plane
Procedures
- Dwyer osteotomy
- Zadek osteotomy
- Calcaneal osteotomies
Advantages
- Minimal soft tissue disruption
- Improved osteotomy mobility
- Reduced need for extensive release
Zadek Osteotomy
Indication
- Insertional Achilles tendinopathy
Procedure
- Dorsal closing wedge osteotomy of calcaneus
Effect
- Moves calcaneal tuberosity away from Achilles insertion
- Reduces tendon tension
MIS in Complex Foot Deformities
Traditional Challenges
- Extensive dissection
- Bone wedge excision
- Foot shortening
- Significant scarring
MIS Advantages
- Controlled wedge resection
- Minimal scarring
- Preservation of soft tissue
Application in Diabetic Foot
Challenges
- Poor soft tissue quality
- Vascular compromise
- Calcified vessels
MIS Benefits
- Small incisions (~3 mm)
- Reduced vascular injury risk
- Precise deformity correction
MIS with External Fixation
Indication
- Severe, multiplanar deformities
Technique
- MIS osteotomy + external fixator (e.g., Taylor Spatial Frame)
Advantages
- Gradual correction
- Rotation and lengthening possible
- Avoids extensive soft tissue dissection
Example: Severe Charcot Deformity
Features
- Ulceration
- Infection
- Severe deformity
Role of MIS
- Enables limb salvage
- Restores plantigrade alignment
- Minimizes complications
Advantages of MIS
- Smaller incisions
- Less soft tissue damage
- Reduced wound complications
- Faster recovery
- Early mobilization
- Improved cosmetic outcomes
- High patient satisfaction
Limitations and Requirements
Learning Curve
- Requires specialized training
- Cadaveric practice recommended
Equipment
- MIS burrs
- Specialized instruments
- Mini C-arm fluoroscopy
Radiation Consideration
- Potential increased exposure without proper optimization
Current Evidence
- MIS is an emerging and rapidly evolving field
- Increasing clinical adoption
- Expanding indications:
- Adult deformity correction
- Pediatric procedures
- Complex reconstructions
Key Take-Home Points
- MIS reduces soft tissue trauma and improves recovery
- Particularly valuable in:
- Forefoot deformities
- Hindfoot osteotomies
- High-risk patients (e.g., diabetics)
- Requires:
- Proper training
- Specialized equipment
- Indications continue to expand with growing evidence

Leave a Reply