Courtesy: Manoj Veetil FRCS Tr and Orth, Birmingham, UK
Metastatic Bone Disease: Practical Principles and Management Pathways
Overview of Metastatic Bone Disease
- Metastatic bone disease is one of the most symptomatic and disabling manifestations of advanced cancer.
- Bone metastases typically occur in a predictable distribution, most commonly involving the spine, pelvis, ribs, and proximal limb girdles.
- Involvement beyond the knee or elbow is uncommon and should raise suspicion for alternative diagnoses.
- Common primary sources include breast, prostate, lung, renal, and thyroid cancers.
- Improved systemic therapies have increased survival in recent years, requiring durable orthopedic management strategies.
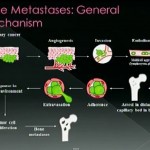
Mechanism and Pathophysiology
- Metastatic lesions weaken bone through osteoclastic activation and local bone destruction.
- Chemical mediators such as transforming growth factor beta stimulate tumor activity and osteoclastic bone resorption.
- Most pathological fractures occur with minimal trauma and are preceded by weeks of prodromal pain.
Clinical Presentation
- Pain is the most common presenting symptom and is typically worse at night.
- Patients may present with pathological fractures following minimal trauma.
- Some patients present with unexplained chronic musculoskeletal pain.
- Occasionally metastatic bone disease may be diagnosed before the primary tumor is identified.
Diagnostic Approach
- A complete history and clinical examination should be followed by targeted investigations.
- Baseline laboratory testing includes routine blood tests, bone profile, liver function tests, tumor markers, and myeloma screening.
- Imaging includes plain radiographs, magnetic resonance imaging of the affected bone, computed tomography of chest, abdomen, and pelvis, and bone scintigraphy.
- Biopsy is required if the diagnosis is uncertain or the primary tumor is unknown.
Differential Diagnosis
- Lesions must be differentiated from primary bone tumors and infection, as treatment differs significantly.
- A solitary lesion should be treated as a primary tumor until proven otherwise.
Risk of Pathological Fracture
- Prophylactic fixation reduces complications compared with treating established fractures.
- Scoring systems such as Mirels score help assess fracture risk but should be interpreted with clinical findings.
- Cortical destruction greater than half of bone diameter suggests high fracture risk.
- Functional pain during daily activities is a strong indication for prophylactic fixation.
Non Surgical Management
- Radiotherapy may relieve pain and promote sclerosis in radiosensitive tumors.
- It is particularly effective in lymphomas, myeloma, breast, and prostate cancers.
- Chemotherapy and endocrine therapy are used depending on tumor type.
- Bisphosphonates and denosumab reduce osteoclastic activity and skeletal complications.
- Other treatments include percutaneous ablation techniques for selected lesions.
Principles of Surgical Management
- Surgical treatment aims to relieve pain, restore mobility, and provide durable stabilization.
- Reconstruction should allow immediate weight bearing and outlast the patient’s life expectancy.
- Bone grafting is generally ineffective in metastatic disease.
- Cement augmentation is frequently used to improve implant stability.
Preoperative Considerations
- Patients require medical optimization including nutritional and anesthetic assessment.
- Bone marrow suppression and coagulation abnormalities are common.
- Hypercalcemia must be corrected before surgery.
- Some tumors such as renal and thyroid metastases are highly vascular and may require preoperative embolization.
- Venous thromboembolism prophylaxis and adequate analgesia are essential.
Site Specific Management
- Proximal femur is commonly affected; options include cemented arthroplasty or endoprosthetic replacement.
- Subtrochanteric lesions often require endoprosthetic reconstruction for durability.
- Diaphyseal lesions are often treated with intramedullary nailing and postoperative radiotherapy.
- Distal femur and proximal tibia lesions may be treated with locking plates and cement augmentation.
- Upper limb lesions are often managed with plating or nailing; joint involvement may require prosthetic replacement.
Pelvic and Acetabular Metastases
- Pelvic disease significantly impacts mobility and quality of life.
- Small acetabular lesions may be managed with cementoplasty.
- Larger lesions require reconstruction techniques to restore weight bearing function.
- Management often involves tumor debulking and structural reconstruction.
Spinal Metastases
- The spine is the most commonly affected site.
- Patients may present with back pain, neurological compromise, or paralysis.
- Magnetic resonance imaging is the investigation of choice.
- Surgery is indicated for instability, neurological compression, radioresistant tumors, and intractable pain.
- Radiotherapy is useful for radiosensitive lesions and selected cases of spinal cord compression.
Treatment Algorithms
- Patients with known malignancy and compatible lesions may proceed directly to treatment after staging.
- Patients without known malignancy require full workup including imaging and biopsy.
- Younger patients require careful evaluation for primary bone tumors.
- Restaging is required in previously treated cancer patients presenting with new lesions.
Key Principles and Outcomes
- Orthopedic management should be integrated into multidisciplinary care.
- Early intervention improves mobility and quality of life.
- Implants must outlast patient survival to avoid revision surgery.
- Failure to intervene appropriately or use durable reconstruction results in poor outcomes.
Discussion Highlights
- Intramedullary nailing remains appropriate for many diaphyseal lesions with reasonable prognosis.
- Endoprosthetic reconstruction is preferred for metaphyseal destruction.
- Positron emission tomography scans are not routinely required but may be useful in selected cases.
Leave a Reply