Courtesy: Dr Dinshaw Pardiwala, Ashok Shyam, Ortho TV
Practical Considerations in Meniscus Repair
Introduction
-
Meniscus injuries are among the most common problems encountered by knee surgeons.
-
Management decisions often depend on multiple factors, including:
-
Patient age
-
Activity level
-
Tear pattern
-
Associated ligament injuries
-
Limb alignment
-
-
Modern practice increasingly emphasizes meniscal preservation rather than meniscectomy, especially in young and active patients.
Case One
Radial Tear of the Lateral Meniscus in a Young Athlete
Clinical Scenario
-
A professional football player presented with:
-
Acute anterior cruciate ligament injury
-
Complete radial tear of the posterior horn of the lateral meniscus
-
Key Surgical Question
-
Should the tear be repaired or partially removed?
Panel Consensus
-
The majority agreed that repair should be attempted.
Rationale for Repair
-
Young patient with traumatic injury
-
Associated anterior cruciate ligament reconstruction improves healing environment
-
Lateral meniscus is critical for load distribution
Repair Techniques Discussed
Possible repair options included:
-
Side-to-side suturing of the radial tear
-
Transosseous pull-out repair similar to root repair techniques
-
Combination of radial repair and root fixation when the tear is close to the root
Expected Healing
-
In young patients with concurrent ligament reconstruction:
-
Healing rates may approach approximately eighty percent.
-
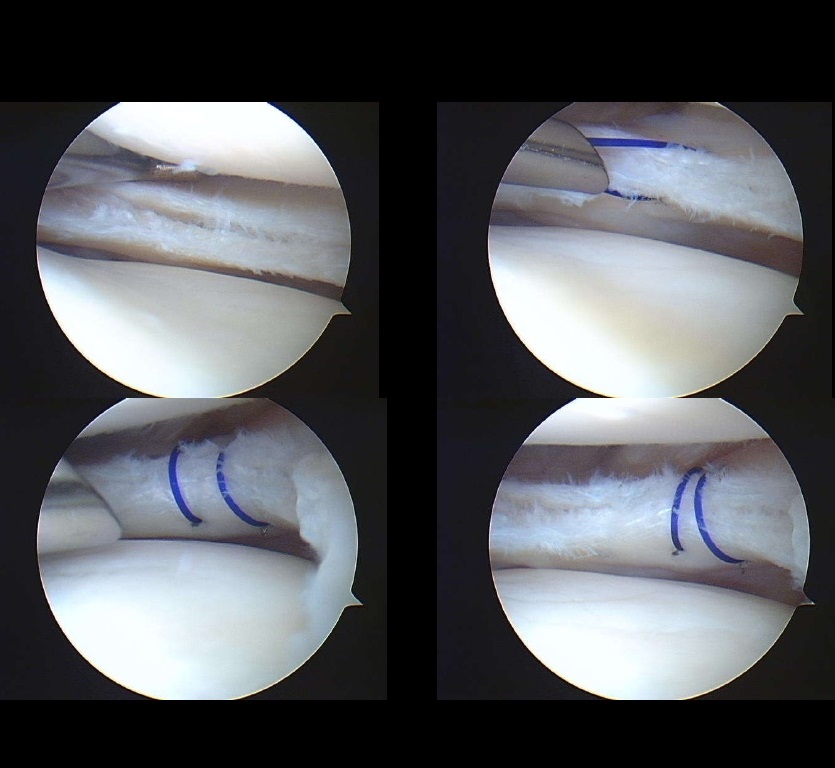
Outcome
-
Second-look arthroscopy performed months later demonstrated:
-
Complete healing of the repaired meniscus
-
Stable fixation with minimal visible sutures
-
Case Two
Tear in the Popliteal Zone of the Lateral Meniscus
Clinical Scenario
-
Patient undergoing anterior cruciate ligament reconstruction
-
Arthroscopy revealed a tear in the popliteal hiatus region of the lateral meniscus.
Surgical Considerations
Key questions included:
-
Whether the tear required repair
-
Whether the popliteus tendon should be included in the repair
Preferred Treatment
-
Arthroscopic repair using all-inside sutures.
Important Technical Points
-
Preparation of the tear bed using rasping or debridement
-
Placement of vertical mattress sutures for stronger fixation
-
Preservation of the popliteus tendon when possible
Healing Potential
-
Healing is enhanced when repair is combined with anterior cruciate ligament reconstruction due to improved biological environment.
Case Three
Complex Lateral Meniscus Tear with Valgus Alignment
Clinical Scenario
-
Young adult presenting with:
-
Lateral knee pain
-
Mechanical symptoms
-
Complex lateral meniscus tear with cyst formation
-
Valgus malalignment
-
Imaging Findings
-
Radial tear component
-
Horizontal cleavage tear
-
Associated parameniscal cyst
Treatment Strategy
Management options included:
-
Arthroscopic meniscus repair
-
Partial meniscectomy
-
Alignment correction through osteotomy
Surgical Decision
-
Partial meniscectomy was performed due to poor tissue quality.
-
Valgus malalignment was corrected with distal femoral osteotomy to reduce lateral compartment load.
Key Principle
-
When meniscal preservation is not feasible, alignment correction may help protect the remaining cartilage and meniscal tissue.
Case Four
Isolated Radial Tear of the Lateral Meniscus
Clinical Scenario
-
Young athlete with:
-
Acute twisting injury
-
Complete radial tear of the lateral meniscus
-
Intact anterior cruciate ligament
-
Surgical Recommendation
-
Strong consensus for repair rather than resection.
Repair Technique
Common techniques include:
-
Combination of inside-out sutures and all-inside fixation devices
-
Multiple sutures placed across the tear to restore hoop stresses
Biological Augmentation
Possible adjuncts discussed:
-
Marrow venting of the intercondylar notch
-
Platelet-rich plasma
-
Fibrin clot augmentation
Rehabilitation
-
Rehabilitation should be slow and protective.
Typical protocol includes:
-
Restricted weight bearing initially
-
Gradual progression of range of motion
-
Return to sports only after several months
Case Five
Discoid Lateral Meniscus with Horizontal Cleavage Tear
Clinical Scenario
-
Adolescent patient with symptomatic discoid lateral meniscus
-
Associated horizontal cleavage tear and parameniscal cyst
Treatment Goals
-
Preserve as much meniscal tissue as possible
-
Restore normal meniscus shape
Surgical Steps
-
Arthroscopic saucerization of the discoid meniscus
-
Decompression of the cyst
-
Repair of the horizontal cleavage tear
Repair Options
Possible repair methods include:
-
Inside-out sutures
-
All-inside devices
-
Horizontal mattress sutures
Important Consideration
-
Excessive meniscectomy in discoid meniscus can lead to early degenerative arthritis, particularly in young patients.
Case Six
Medial Meniscus Root Tear
Clinical Scenario
-
Middle-aged patient with sudden onset knee pain after minor activity
-
Imaging demonstrated a posterior medial meniscus root tear with meniscal extrusion.
Typical Clinical Features
-
Sudden pain during low-impact activity
-
Difficulty bearing weight
-
Progressive symptoms over time
Surgical Management
-
Arthroscopic root repair using transosseous pull-out technique.
Suture Techniques
Common methods include:
-
Suture tape fixation
-
Luggage-tag configuration
-
Fixation over a cortical button on the tibia
When to Add an Osteotomy
Osteotomy may be considered when:
-
Significant varus malalignment exists
-
Medial compartment overload is present
-
Meniscal repair alone may fail due to abnormal load
However, in patients with normal alignment, isolated root repair is generally performed first.
Influence of Osteoarthritis
Decision-making should consider cartilage status:
-
Mild osteoarthritis: repair may still be beneficial
-
Advanced osteoarthritis: repair may provide limited benefit
Case Seven
Degenerative Horizontal Meniscus Tear
Clinical Scenario
-
Middle-aged patient with degenerative medial meniscus tear and cyst
Management Strategy
Treatment may include:
-
Limited partial meniscectomy to remove unstable tissue
-
Cleaning of the cleavage plane
-
Meniscus repair when feasible
Healing Considerations
-
Degenerative tears have lower healing potential compared with traumatic tears.
-
Biological augmentation techniques may be considered to improve healing.
Rehabilitation Principles
Rehabilitation protocols vary depending on tear pattern and repair type.
Radial Tears
-
Non-weight bearing for several weeks
-
Gradual return to full activity over several months
Root Repairs
-
Protected weight bearing for approximately six weeks
-
Avoid deep flexion for several months
Return to Sports
-
Typically delayed until adequate strength, motion, and functional testing are achieved.
Key Principles of Modern Meniscus Surgery
-
Meniscal preservation should be attempted whenever possible.
-
Repair is favored in young, active patients with traumatic tears.
-
Tear pattern and tissue quality strongly influence repair success.
-
Limb alignment and cartilage health must be considered during surgical planning.
-
Rehabilitation plays a critical role in protecting the repair and restoring function.
Leave a Reply