Medial Retinaculum Plasty Versus Medial Patellofemoral Ligament Reconstruction for Recurrent Patellar Instability in Adults: A Randomized Controlled Trial
Long-Fei Ma, M.D., Fei Wang, Ph.D., Bai-Cheng Chen, Ph.D., Cheng-Hai Wang, M.D.,
Jian-Wei Zhou, M.D., and Hao-Yu Wang, M.D.
From the Department of Joint Surgery, Third Hospital of Hebei Medical
University, Shijiazhuang, China.
Arthroscopy. 2013 May;29(5):891-7. doi: 10.1016/j.arthro.2013.01.030. Epub 2013 Apr 6.
- There are many procedures described for the treatment of Recurrent Patellar Dislocation/ Instability. In a study published in Arthroscopy Journal 70 patients with recurrent patellar instability were randomized to receive medial retinaculum plasty(MRP) or medial patellofemoral ligament reconstruction.
- Normally there is a 15 to 45 % recurrence rate when patellar dislocation is treated conservatively. Medial Retinaculum Plasty uses realignment based on anatomic, biochemical and MR imaging based research.
- In this study Ma et al.. compared the results of MRP against MPFL reconstruction with concomitant lateral release in 70 patients.
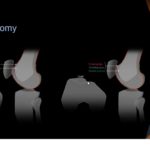
Technique of Medial Retinaculum Plasty:
- Transverse dissection is made along the junction line of the vastus medialis and medial retinaculum to the medial femoral condyle to separate the 2 adjacent sections.
- The separated medial retinaculum (including the MPFL) is sutured proximally and laterally near the upper pole of the patella temporarily.
- The vastus medialis is then sutured distally and laterally to the midline of the patella
Methods (PICO):
- Population: 70 patients with recurrent instability.
- Intervention: MRP group mean age 28 years (n=31)
- Comparison: MPFL recon group mean age 28.4 years (n=32)
- Outcome measurement: CT scan for patellar angle restoration. Apprehension test Kujala score, Tegner activity score and subjective questionnaire.
- Type of study: Level 2 therapeutic randomized control trial.
- Inclusion critera: All patients had more than 2 episodes of dislocation or 1 episode of dislocation plus multiple episodes of instability
- Exclusion criteria: MPFL injury at the femoral insertion, which was found by the MRI scan; previous surgery for patellar instability and displaced fractures of the patellar or lateral femoral condyle that were confirmed by CT examinations; a sulcus angle greater than 150 degree; a tibial tuberosity trochlear groove distance greater than 15 mm; severe femoral anteversion (>35 degree) or valgus knee (>5 degree); knee symptoms in the contralateral leg; and knee cruciate ligament or collateral ligament injury
- Average follows up period: 40 months
- Results: In both groups the congruence angle, patellar tilt and patellar lateral shift angle decreased to normal. Median Kujala scores and median Tegner activity scores improved in both groups.
- Conclusion: Medial Retinaculum Plasty (MRP) is a very useful technique for the treatment of patellar instability. MRP provides both dynamic and static stability for the patella due the overlapping features of the VMO (Vastus Medialis Obliquus) and Medial Patellofemoral Ligament(MPFL). MRP could achieve similar results as MPFL Reconstruction for the treatment of Patellar Instability due to MPFL injuries from the patella and midsubstance tears
Ref:
- http://www.arthroscopyjournal.org/article/S0749-8063%2813%2900096-0/abstract
- http://www.ncbi.nlm.nih.gov/pubmed/23566568
- http://www.myorthoevidence.com/?section=15&id=5016&list=16
Leave a Reply