Courtesy: Dr Strickland, Ashok Shyam TV, Ortho
Changing Perspective
-
Repair of medial meniscus root tears has gained momentum only in the last several years.
-
Historically, many of these tears—especially in middle-aged patients—were treated nonoperatively or with meniscectomy.
-
These are sometimes referred to as “underserved tears” because they were frequently missed or undertreated.
The key questions:
-
Which tears should not be fixed?
-
If operative, how should they be repaired?
Typical Clinical Presentation
Common patient profile:
-
Age: 40 to 50 years.
-
Low-energy injury (for example, stepping into a bathtub).
-
Sudden posterior knee pain.
-
Sensation of instability or buckling.
-
Normal radiographs.
Magnetic resonance imaging typically shows:
-
Detachment of the posterior horn of the medial meniscus from its root.
-
“Ghost sign” on sagittal sequences.
-
Increased signal on fat-suppressed images.
Important tip:
Always review fat-suppressed sequences carefully. Root tears are commonly missed.
Preoperative Considerations
Before offering repair:
-
Evaluate articular cartilage.
-
Advanced arthritis predicts failure.
-
-
Assess alignment.
-
Counsel the patient that:
-
Repair may not be possible.
-
Surgery may be abandoned intraoperatively if arthritis is severe.
-
Healing is not guaranteed.
-
Intraoperative Principles
1. Optimize Visualization
-
Perform medial collateral ligament pie-crusting if needed.
-
Adequate exposure is essential.
-
Poor visualization compromises repair quality.
2. Prepare the Footprint
-
Debride the root attachment site.
-
Curette to bleeding bone.
-
Create a biologically favorable surface for healing.
-
Soft tissue-to-bone healing is the goal.
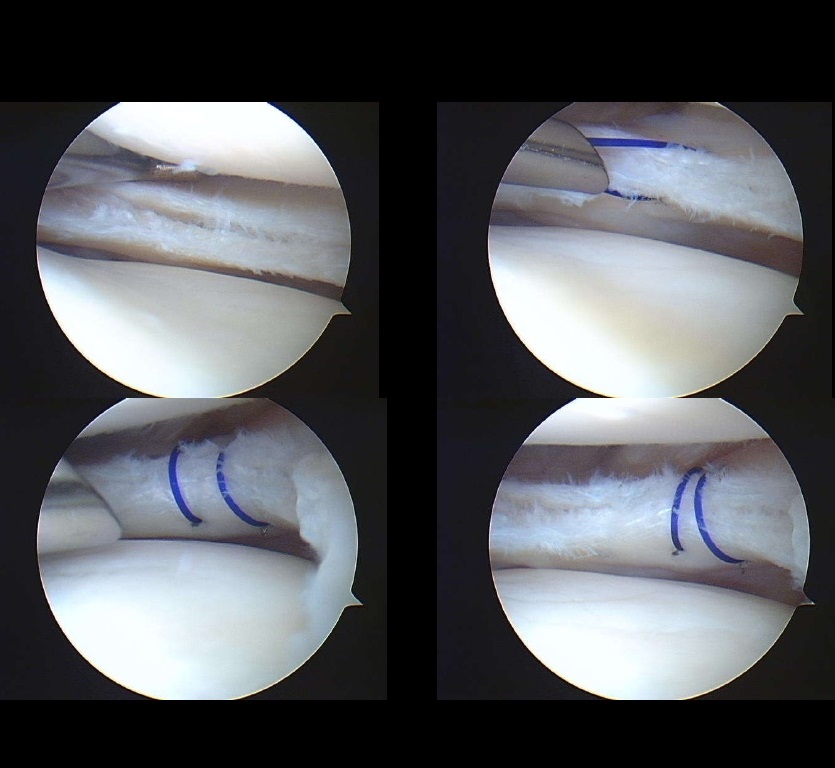
3. Suture Passage
Multiple techniques are acceptable:
-
High-strength suture tape.
-
Luggage-tag configuration.
-
Simple stitch.
-
Mattress stitch.
Key requirement:
-
Meniscal tissue must be strong enough to hold sutures.
-
Poor tissue quality may require abandoning repair.
Surgeon preference varies:
-
Single-use or reusable suture passers.
-
All-in-one passing systems.
-
Loop-based suture constructs.
4. Tunnel Creation
Options include:
-
Standard anterior cruciate ligament tibial guide.
-
Root-specific tibial guide (easier posterior positioning).
Challenges:
-
Standard guides may not reach far enough posterior.
-
Dedicated guides improve accuracy.
After guide placement:
-
Drill tibial tunnel exiting at anatomic root footprint.
5. Fixation Methods
Several fixation strategies exist:
-
Tie sutures over a cortical button.
-
Bone bridge with dual tunnels.
-
Interference screw fixation.
-
Anchor-based footprint fixation.
Before final fixation:
-
Confirm adequate tension arthroscopically.
-
Ensure meniscus is well reduced to footprint.
-
Avoid under-tensioning.
Postoperative Protocol
-
Non–weight bearing for six weeks.
-
Increased risk of deep vein thrombosis.
-
Gradual return to activity thereafter.
Healing Rates and Expectations
Second-look arthroscopy studies show:
-
Approximately 70 percent healing rate.
Important patient counseling points:
-
Repair may not heal.
-
Symptom improvement is common even if healing is incomplete.
-
Long-term goal is joint preservation.
Biomechanical Rationale
Meniscus root tears function similarly to total meniscectomy:
-
Loss of hoop stress.
-
Increased tibiofemoral contact pressures.
-
Accelerated cartilage degeneration.
Biomechanical studies demonstrate:
-
Restoring the root to its footprint improves contact mechanics.
-
More anatomic reduction yields better load distribution.
Effect on Osteoarthritis Progression
Evidence suggests:
-
Lower progression to osteoarthritis compared with nonoperative management or meniscectomy.
-
Example data:
-
Approximately 29 percent progression after repair.
-
Approximately 39 percent without repair.
-
Although not completely protective, repair reduces risk.
Cost-Effectiveness
Studies indicate:
-
Root repair may be cost-effective long term.
-
Reduced progression to knee arthroplasty.
-
Lower overall lifetime treatment costs.
As healthcare systems emphasize value-based care, this becomes increasingly relevant.
When Not to Repair
Consider avoiding repair if:
-
Advanced medial compartment osteoarthritis.
-
Severe cartilage loss.
-
Poor tissue quality.
-
Significant malalignment without corrective osteotomy.
Key Takeaways
-
Medial meniscus root tears are frequently missed.
-
Fat-suppressed magnetic resonance imaging sequences improve detection.
-
Advanced arthritis predicts failure.
-
Adequate exposure and footprint preparation are essential.
-
Tissue quality determines feasibility.
-
Repair improves contact mechanics.
-
Approximately 70 percent healing rate.
-
Reduces risk of osteoarthritis progression.
-
Non–weight bearing protocol required.
-
Not every root tear is repairable.
Leave a Reply