Courtesy: Scott Kozin, Dan Zlotolow, Shirner’s hospital for Children, USA
Medial Epicondyle Fracture Fixation (Pediatric) – Stepwise Approach
1. Indications for Surgery
Absolute / Strong Indications
- Fragment incarcerated in the joint
- Associated elbow dislocation
- Ulnar nerve symptoms
Relative Indications
- Displacement >5 mm (controversial threshold)
- Elbow instability (valgus instability)
- High-demand patients:
- Throwing athletes
- Weight-bearing upper limb
2. Patient Positioning
Position
- Lateral decubitus position
Advantages
- Gravity provides:
- Varus force – aids reduction
- Improved exposure of medial elbow
- Easier fluoroscopic imaging
Arm Position
- Hand placed on hip
- Improves fracture reduction
3. Surgical Steps
A. Preparation
- Apply tourniquet
- Use fluoroscopy to confirm:
- Displacement
- Valgus instability
B. Incision
- Curvilinear incision
- Positioned:
- Posterior to medial epicondyle
C. Exposure
- Perform blunt dissection
- Clear fracture site:
- Remove hematoma
- Remove soft tissue interposition
D. Ulnar Nerve Handling
- Identify and protect ulnar nerve
- Mobilize if necessary
E. Fracture Reduction
- Free fragment from adhesions
- Achieve anatomical reduction
F. Provisional Fixation
- Insert one K-wire
- Confirm position with fluoroscopy
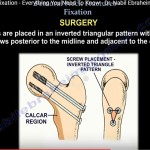
G. Definitive Fixation
Stepwise Technique
- Insert second K-wire (derotation pin)
- Measure depth – determine screw length
- Clear soft tissue from bone surface
- Replace K-wire with guide wire
- Insert cannulated screw
Important Precaution
- Avoid over-tightening:
- Prevents fragment comminution
H. Final Fixation Check
- Remove derotation wire
- Confirm using fluoroscopy:
- Stability
- Screw position
I. Soft Tissue Closure
- Repair soft tissues over screw
- Close any tears
J. Range of Motion Assessment
- Perform intraoperative movement
Ensure
- No impingement
- No irritation of ulnar nerve
4. Postoperative Care
Immobilization
- Bivalved long arm cast
- Duration:
- ~4 weeks
Follow-Up
At 4 Weeks
- Assess fracture healing
- Remove pins (if used)
At 8 Weeks
- Evaluate:
- Range of motion
5. Outcomes
- Generally:
- Good fracture healing
Early Phase
- Mild restriction in ROM possible
Long-Term
- Gradual recovery expected
6. Key Exam Pearls
- Always protect ulnar nerve
- Lateral decubitus position:
- Provides varus reduction advantage
- Use derotation pin before screw fixation
- Avoid over-tightening screws
- Always check range of motion intraoperatively
Final Message
- Successful fixation depends on:
- Precise reduction
- Careful handling of the ulnar nerve
- Stable fixation with proper technique

Leave a Reply