Courtesy: Prof Wolf Petersen, Martin Luther Krakenhaus, Berlin, Germany
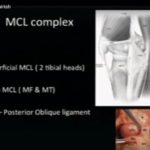
Anatomy of the Medial Collateral Ligament Complex
The medial side of the knee consists of three principal ligamentous structures:
1. Superficial Medial Collateral Ligament
-
Origin: Medial femoral epicondyle
-
Insertion: Approximately 7–8 centimeters distal to the joint line, below the pes anserinus
-
Function:
-
Primary restraint to valgus stress
-
Contributes to control of rotational stability
-
2. Posterior Oblique Ligament
-
Runs obliquely from the posterior medial femoral condyle to the posterior medial tibia
-
Functions:
-
Secondary restraint to posterior tibial translation
-
Stabilizer against valgus stress, especially in knee extension
-
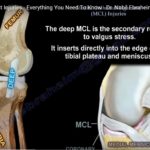
3. Deep Medial Collateral Ligament (also described by some as the anterior oblique ligament)
-
Connects the femur to the proximal medial tibia
-
Functions:
-
Important restraint to anterior tibial translation
-
Contributes to valgus and external rotational stability
-
Additional medial structures:
-
Posterior capsule
-
Coronary ligament (connecting medial meniscus to tibia), relevant in ramp-type lesions
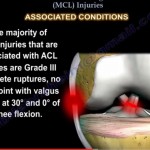
Classification of Medial Collateral Ligament Injuries
Medial collateral ligament injuries are traditionally classified into three grades:
Grade I
-
Stretch injury with minimal fiber disruption
-
Firm end point
-
No increased joint laxity
Grade II
-
Partial tear
-
Firm end point
-
Mild to moderate valgus laxity
Grade III
-
Complete tear
-
No firm end point
-
Marked valgus laxity
Healing Potential and Nonoperative Treatment
-
The medial collateral ligament has good intrinsic healing potential.
-
Clinical research has shown:
-
Isolated Grade I and II injuries respond well to nonoperative treatment.
-
Many Grade III isolated superficial ligament tears may also heal with bracing.
-
In combined anterior cruciate ligament and medial collateral ligament injuries, nonoperative treatment of the medial side has shown acceptable outcomes in selected cases.
-
However, not all Grade III injuries behave similarly.
Special Injury Pattern: Distal “Stener-like” Lesion
-
Occurs when the distal superficial medial collateral ligament avulses and displaces above the pes anserinus.
-
The displaced stump loses contact with bone.
-
Healing potential is poor without surgical intervention.
Management:
-
Surgical repair using suture anchor fixation.
-
High return-to-sport rates have been reported following repair of these lesions.
Indications for Surgical Treatment in Acute Injuries
Nonoperative Treatment Recommended For:
-
Grade I injuries
-
Grade II injuries
-
Isolated Grade III superficial medial collateral ligament tears without multi-structure involvement
Surgical Treatment Recommended For:
-
Distal avulsion with interposition (Stener-like lesion)
-
Proximal avulsions with gross instability
-
Combined injury of:
-
Superficial medial collateral ligament
-
Posterior oblique ligament
-
Posteromedial capsule
-
-
Knee dislocations involving medial structures
-
Multi-ligament injuries
Acute Multi-Ligament Knee Injuries
Initial Priorities:
-
Vascular assessment
-
Neurological examination
-
Magnetic resonance imaging
If vascular injury is present:
-
Immediate vascular management
If no vascular injury:
-
Imaging-guided surgical planning
Surgical Strategy:
-
Bony avulsions ? Anchor fixation
-
Peripheral ligament tears ? Suture repair
-
Intraligamentous tears ? Repair with augmentation (suture tape or graft)
-
Severe tissue destruction ? Consider graft augmentation
Repair Techniques in Acute Setting
1. Anchor Refixation
-
Preferred for proximal or distal avulsions
-
Soft anchors commonly used
2. Suture Repair
-
For intraligamentous tears
-
Often augmented with:
-
Internal brace (suture tape)
-
Graft augmentation in severe cases
-
Chronic Medial Instability
Chronic instability may result from:
-
Delayed treatment
-
Failed healing
-
Multi-ligament trauma
-
Untreated vascular emergencies
If instability persists beyond 6 to 12 weeks, reconstruction is generally indicated.
Reconstruction Techniques
1. Plication Technique
-
Advancement and tightening of native tissue
-
Historically described but less commonly used today
2. Tenodesis Techniques
-
Use of pedicled semitendinosus tendon
-
Non-anatomic reconstruction
-
May compromise medial hamstring function
3. Anatomic Reconstruction Techniques (Preferred)
a. Superficial Medial Collateral Ligament Reconstruction
-
Femoral and tibial tunnels placed at anatomic insertion sites
b. Posteromedial Reconstruction
-
Reconstruction of:
-
Superficial medial collateral ligament
-
Posterior oblique ligament
-
c. Anteromedial Reconstruction
-
Reconstruction of:
-
Superficial medial collateral ligament
-
Deep medial collateral ligament
-
Why Preserve Ipsilateral Hamstrings?
Biomechanical research has shown:
-
Medial hamstrings act as dynamic stabilizers against valgus and rotational stress.
-
Preserving ipsilateral hamstrings may improve functional outcomes in medial instability.
Graft Choices for Reconstruction
Medial reconstructions require long tubular grafts.
Options include:
-
Contralateral semitendinosus tendon
-
Peroneus longus split graft
-
Rectus femoris tendon
-
Tubular allografts
Ipsilateral hamstrings are preferably preserved when possible.
Clinical Evaluation of Chronic Instability
Important examination findings include:
-
Increased medial joint opening compared to lateral side
-
Positive valgus stress test
-
Positive dial test
-
Anteromedial rotational instability
-
Posterior drawer that increases in internal rotation (suggesting posterior oblique ligament involvement)
Stress radiographs:
-
Medial joint space widening
-
Posterior translation greater than 12 millimeters may indicate additional posteromedial or posterolateral injury
Indications for Adding Posterior Oblique Ligament Reconstruction
-
Posterior drawer increases in internal rotation
-
Combined posterior cruciate ligament injury
-
Clinical evidence of posteromedial instability
-
Severe medial laxity in extension
Routine reconstruction is not necessary for every Grade III medial collateral ligament tear. Decision depends on associated instability pattern.
Acute Repair Versus Reconstruction
-
Many surgeons favor repair in the acute setting when tissue quality permits.
-
Repair allows preservation of native tissue.
-
Reconstruction is considered in:
-
Severe tissue destruction
-
Poor tissue quality
-
Failed prior repair
-
Key Practical Points
-
Tibial avulsions respond well to anchor repair.
-
Intraligamentous tears may require augmentation.
-
Multi-ligament injuries demand careful assessment of rotational instability.
-
Chronic instability is best managed with anatomic reconstruction techniques.
-
Long tubular grafts are required for medial reconstruction.
-
Preservation of ipsilateral hamstrings is advisable when feasible.
Summary
-
Most Grade I and II medial collateral ligament injuries heal without surgery.
-
Selected Grade III injuries can also be treated nonoperatively.
-
Stener-like distal avulsions require surgical repair.
-
Multi-structure and knee dislocation injuries require surgical management.
-
Chronic instability should be treated with anatomic reconstruction tailored to the instability pattern.

Leave a Reply