Courtesy: Dr Andy Williams, Ashok Shyam, Ortho TV
Understanding the Medial Collateral Ligament in Knee Stability
Introduction
-
Research over recent years has focused on improving the understanding of the medial collateral ligament of the knee.
-
The goal has been to study three key aspects:
-
Detailed anatomy
-
Biomechanics
-
Surgical techniques for injury management
-
-
These studies have helped refine treatment strategies for medial knee instability.
Anatomical Structure of the Medial Collateral Ligament
Components of the Medial Collateral Ligament
The medial collateral ligament complex consists of several distinct parts:
-
Superficial medial collateral ligament
-
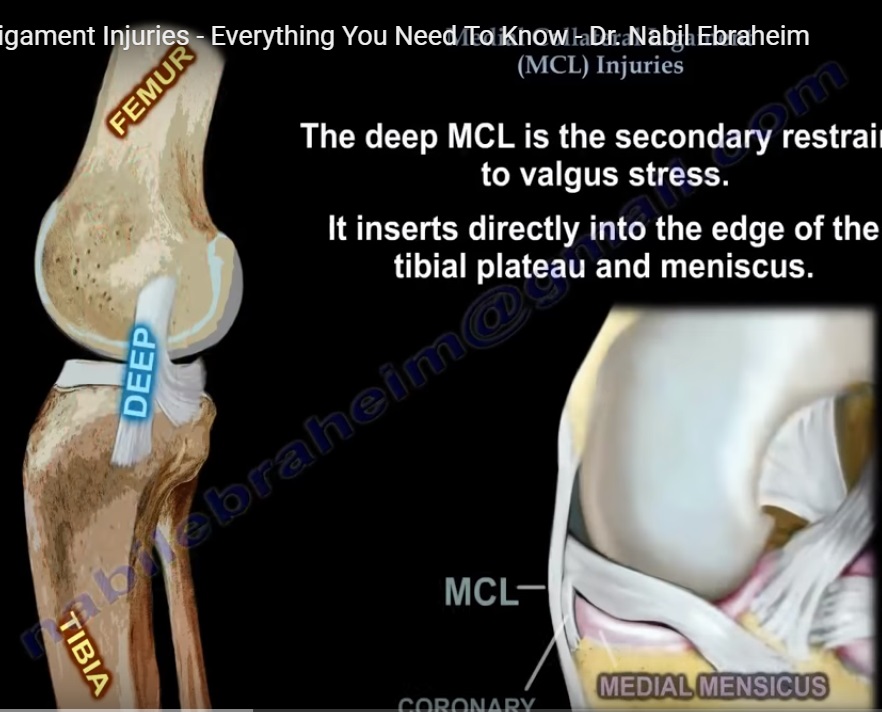
Deep medial collateral ligament
-
Posterior oblique ligament
Each component contributes differently to knee stability.
Attachment Sites
-
The superficial medial collateral ligament attaches proximally near the medial femoral epicondyle.
-
The deep medial collateral ligament attaches more posteriorly and distally along the tibia.
-
The ligament fibers spread in a fan-shaped configuration, especially as they extend distally.
Orientation of Fibers
-
The fibers of the deep medial collateral ligament run in an oblique direction.
-
The anterior portion of the ligament is particularly important for resisting external rotation of the tibia.
Biomechanical Role of the Medial Collateral Ligament
Biomechanical studies using robotic testing systems have helped determine how each ligament component contributes to knee stability.
Key Findings
Anterior Tibial Translation
-
The primary restraint is the anterior cruciate ligament.
Valgus Stability
-
The superficial medial collateral ligament is the main stabilizer against valgus stress throughout the range of motion.
External Rotation Stability
-
Contrary to earlier beliefs, the deep medial collateral ligament plays the most important role in controlling external rotation between zero and ninety degrees of knee flexion.
Anteromedial Rotatory Instability
Mechanism
Anteromedial rotatory instability occurs when:
-
The tibia translates forward relative to the femur.
-
The instability occurs predominantly on the medial side of the knee.
-
External rotational forces increase stress on the anterior cruciate ligament.
Effect of Medial Collateral Ligament Injury
Biomechanical studies have shown that:
-
When external rotational torque is applied to the knee, tension develops in the anterior cruciate ligament.
-
If the medial collateral ligament is deficient, the stress on the anterior cruciate ligament increases significantly.
Clinical studies suggest that anterior cruciate ligament graft failure rates increase when medial collateral ligament laxity is not treated appropriately.
Indications for Surgical Treatment
Most medial collateral ligament injuries heal well without surgery.
However, surgical treatment may be considered in the following situations:
Persistent Medial Opening in Full Extension
-
Indicates severe ligament insufficiency.
Positive Dial Test
-
Suggests medial rotatory instability.
Stener-Type Lesion
-
Occurs when the tibial attachment of the superficial medial collateral ligament becomes trapped above the hamstring tendons.
Ligament Interposition in the Joint
-
When the torn ligament folds into the joint space.
Combined Ligament Injuries
-
Especially when associated with anterior cruciate ligament reconstruction.
Persistent Instability After Bracing
-
If significant laxity remains after approximately three months of conservative treatment.
High-Demand Athletes
-
In competitive athletes with combined injuries, earlier surgical intervention may be considered.
Principles of Surgical Management
Anatomical Restoration
The primary goal of surgery is to restore the natural anatomy of the medial structures.
Acute Injuries
-
Preferably treated with direct repair using sutures or suture anchors.
Chronic Injuries
-
May require ligament tightening and reconstruction procedures.
Layered Surgical Approach
The medial side of the knee contains multiple tissue layers.
Surgical repair may involve:
-
Splitting the superficial fascial layer.
-
Exposing the superficial medial collateral ligament.
-
Accessing and tightening the deep medial collateral ligament using capsular shift techniques.
Reconstruction Techniques
Many reconstruction techniques use hamstring grafts.
However, concerns exist because:
-
The medial collateral ligament is a large complex structure.
-
Replacing it with one or two small grafts may not accurately reproduce its anatomy.
Therefore, reconstruction is often used to protect the repaired ligament rather than replace it entirely.
Role of Reconstruction
Reconstruction serves mainly to:
-
Protect the repaired ligament during healing.
-
Allow early knee movement and rehabilitation.
-
Prevent excessive stress on healing tissues.
Once healing occurs, the reconstruction graft becomes less important.
Posterior Oblique Ligament Reconstruction
Posterior oblique ligament reconstruction is not routinely necessary.
It may be considered in cases such as:
-
Posteromedial rotatory instability
-
Excessive knee hyperextension associated with medial injury
However, these situations are relatively uncommon.
Biomechanical Research on Reconstruction Techniques
Research comparing different reconstruction strategies has revealed important insights.
Single Graft Reconstructions
-
Often restore valgus stability.
-
May not adequately control rotational instability.
Reconstructions Including Deep Medial Collateral Ligament
-
Provide better control of both valgus and rotational instability.
Short Isometric Reconstruction Concept
An alternative reconstruction approach involves:
-
Using a short graft placed between the femoral epicondyle and proximal tibia.
-
Ensuring the graft position remains isometric throughout knee movement.
Advantages include:
-
Reduced graft stretching
-
Improved rotational control
-
Strong fixation due to better bone quality in the proximal tibia
Surgical Technique Considerations
Key technical points include:
-
Accurate placement of guide pins at anatomical landmarks.
-
Testing graft isometry through knee flexion and extension.
-
Adjusting femoral placement if graft tension changes during motion.
Clinical Outcomes
Clinical studies involving athletes with combined ligament injuries have demonstrated encouraging results:
-
Approximately ninety percent of athletes returned to professional sport.
-
Around eighty five percent returned to their previous level of competition.
Nonoperative Treatment
Most medial collateral ligament injuries do not require surgery.
Standard nonoperative treatment includes:
Initial Phase (First Two Weeks)
-
Knee bracing between thirty and sixty degrees.
-
Non weight bearing.
Intermediate Phase
-
Gradual increase in knee motion.
-
Partial weight bearing.
Final Phase
-
Full weight bearing with brace support.
Biological therapies such as platelet-rich plasma may be considered in certain chronic cases.
Example of Successful Nonoperative Treatment
A high-level athlete sustained a severe knee injury involving:
-
Anterior cruciate ligament rupture
-
Grade three medial collateral ligament injury
-
Partial posterior cruciate ligament injury
-
Lateral ligament injuries
-
Meniscal tears
-
Osteochondral fracture
Treatment strategy included:
-
Surgical repair of the lateral structures and meniscus.
-
Bracing to allow healing of the medial and posterior ligaments.
-
Delayed anterior cruciate ligament reconstruction.
The athlete eventually returned to elite competition and achieved international success.
Key Takeaways
-
The medial collateral ligament complex plays a crucial role in knee stability.
-
The deep medial collateral ligament is particularly important for controlling external rotation.
-
Not all medial collateral ligament injuries require surgery.
-
When surgery is necessary, the goal should be anatomic repair supported by reconstruction when needed.
-
Reconstruction is often performed to protect healing tissues rather than to fully replace the native ligament.


Leave a Reply