Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Mallet Finger
Overview
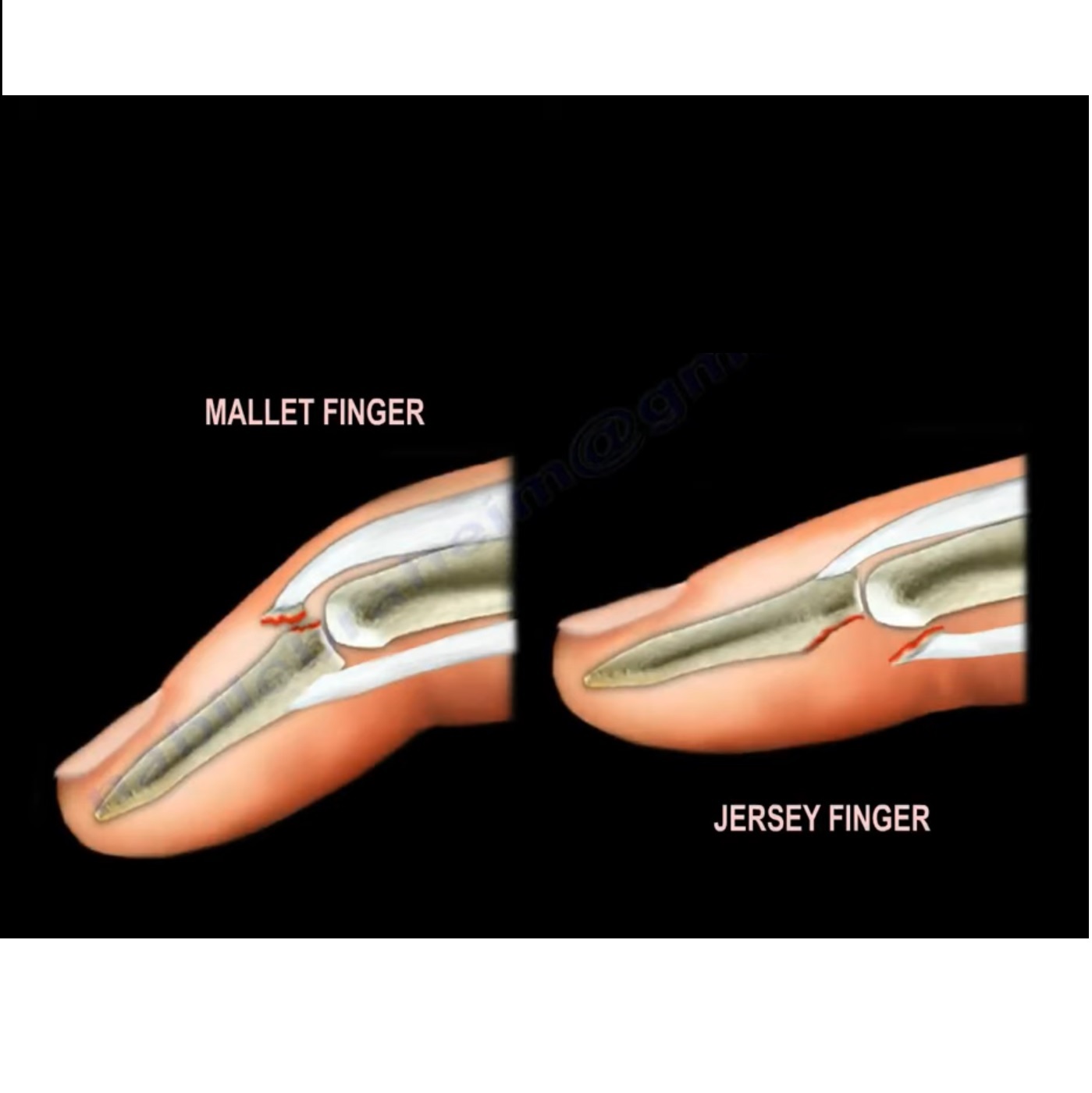
- Mallet finger is caused by disruption of the terminal extensor tendon at the distal interphalangeal (DIP) joint
- Results in inability to actively extend the DIP joint
- Injury may be:
- Pure tendon rupture
- Bony avulsion fracture at base of distal phalanx
Comparison Injury: Jersey Finger
Mallet Finger
- Extensor tendon injury
- Dorsal aspect of finger
- Inability to extend DIP joint
Jersey Finger
- Flexor digitorum profundus (FDP) avulsion
- Volar aspect of finger
- Inability to flex DIP joint
Relevant Anatomy
- Terminal extensor tendon inserts at base of distal phalanx
- Injury at insertion causes loss of active DIP extension
Mechanism of Injury
- Forced flexion of extended fingertip
- Common in ball sports:
- Baseball
- Football
- Volleyball
Most commonly affected fingers:
- Long finger
- Ring finger
- Small finger
Usually involves dominant hand
Clinical Features
- Inability to actively extend DIP joint
- DIP rests in flexion
- Characteristic drooping fingertip appearance
Types of Mallet Finger
1. Tendinous Mallet Finger
- Pure extensor tendon rupture
- No fracture
2. Bony Mallet Finger
- Avulsion fracture at base of distal phalanx
3. Mallet Fracture with Subluxation
- Larger fracture fragment
- Associated volar subluxation of distal phalanx
Radiological Findings
X-ray may show:
- Avulsion fragment at base of distal phalanx
- Size of articular involvement
- Volar subluxation of distal phalanx in severe injuries
Conservative Management
Mainstay of Treatment
- Continuous DIP splinting in extension
Duration:
- Typically 6–8 weeks
Important principles:
- Splint must remain on continuously
- Even brief DIP flexion can disrupt healing
Splint Types
- Dorsal splint
- Volar splint
Key Rehabilitation Principle
- Proximal interphalangeal (PIP) joint should remain mobile
Purpose:
- Prevent stiffness
- Reduce risk of swan neck deformity
Delayed Presentation
- Injuries presenting up to 4 weeks later can still be treated successfully with splinting
Indications for Surgery
Absolute / Common Indications
- Volar subluxation of distal phalanx
- Large bony fragment involving >50% of articular surface
Relative Indications
- Some surgeons use >30% articular involvement
- Failure of conservative treatment
- Selected patient preference
Surgical Techniques
Treatment Goal
- Maintain DIP extension until healing occurs
Percutaneous Pinning
Tendon Injuries
- Single pin fixation may be adequate
Fracture Injuries
- Extension block pinning commonly used
Technique:
- Extension block wire inserted
- DIP extended to reduce fragment
- Additional fixation maintains alignment
Outcomes
- Mild extensor lag may persist
- Usually minimal functional limitation
Complications
Residual Extensor Lag
- Common minor complication
- Often cosmetically noticeable only
Swan Neck Deformity
Mechanism:
- DIP flexion with compensatory PIP hyperextension
Prevention:
- Proper splinting
- Maintain free PIP motion
Other Complications
- Joint stiffness
- Skin irritation from splint
- Recurrent deformity
Key Clinical Pearls
- Most mallet fingers treated non-operatively
- Continuous splint compliance is critical
- PIP joint should remain free
- Delayed presentation can still respond to splinting
- Surgery mainly indicated for:
- Subluxation
- Large articular fractures
- Mild residual lag usually does not affect function



Leave a Reply