Courtesy: Prof Nabil EBraheim, University of Toledo, Ohio, USA
Definition
Maisonneuve fracture is a proximal fibular fracture associated with an unstable syndesmotic injury of the ankle.
It is an important injury because the ankle injury may appear minor while significant instability exists at the syndesmosis.
Why is it Commonly Missed?
The injury may present without:
- Lateral malleolus fracture
- Medial malleolus fracture
As a result:
- The injury may be misdiagnosed as a simple ankle sprain.
- The proximal fibular fracture may be overlooked.
- Patients may be treated for an isolated fibular fracture while the unstable ankle injury remains undiagnosed.
A high index of suspicion is essential.
Important Clinical Principle
Maisonneuve fracture = Syndesmotic injury
Syndesmotic injury = Syndesmotic reduction and fixation
Clinical Examination
Always examine the entire leg in patients with ankle injuries.
Look for
- Tenderness over the proximal fibula
- Medial ankle pain
- Syndesmotic tenderness
- Ankle instability
Clinical Tests
Squeeze Test
Compression of the tibia and fibula at the mid leg produces pain at the syndesmosis.
External Rotation Stress Test
External rotation of the foot reproduces syndesmotic pain.
Both tests suggest syndesmotic injury.
When Should You Obtain Long Leg Radiographs?
If ankle radiographs demonstrate:
- Medial malleolus fracture
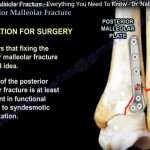
- Posterior malleolus fracture
- Medial clear space widening without a lateral malleolus fracture
Then obtain:
- Full length tibia fibula radiographs
- Imaging that includes both the knee and ankle
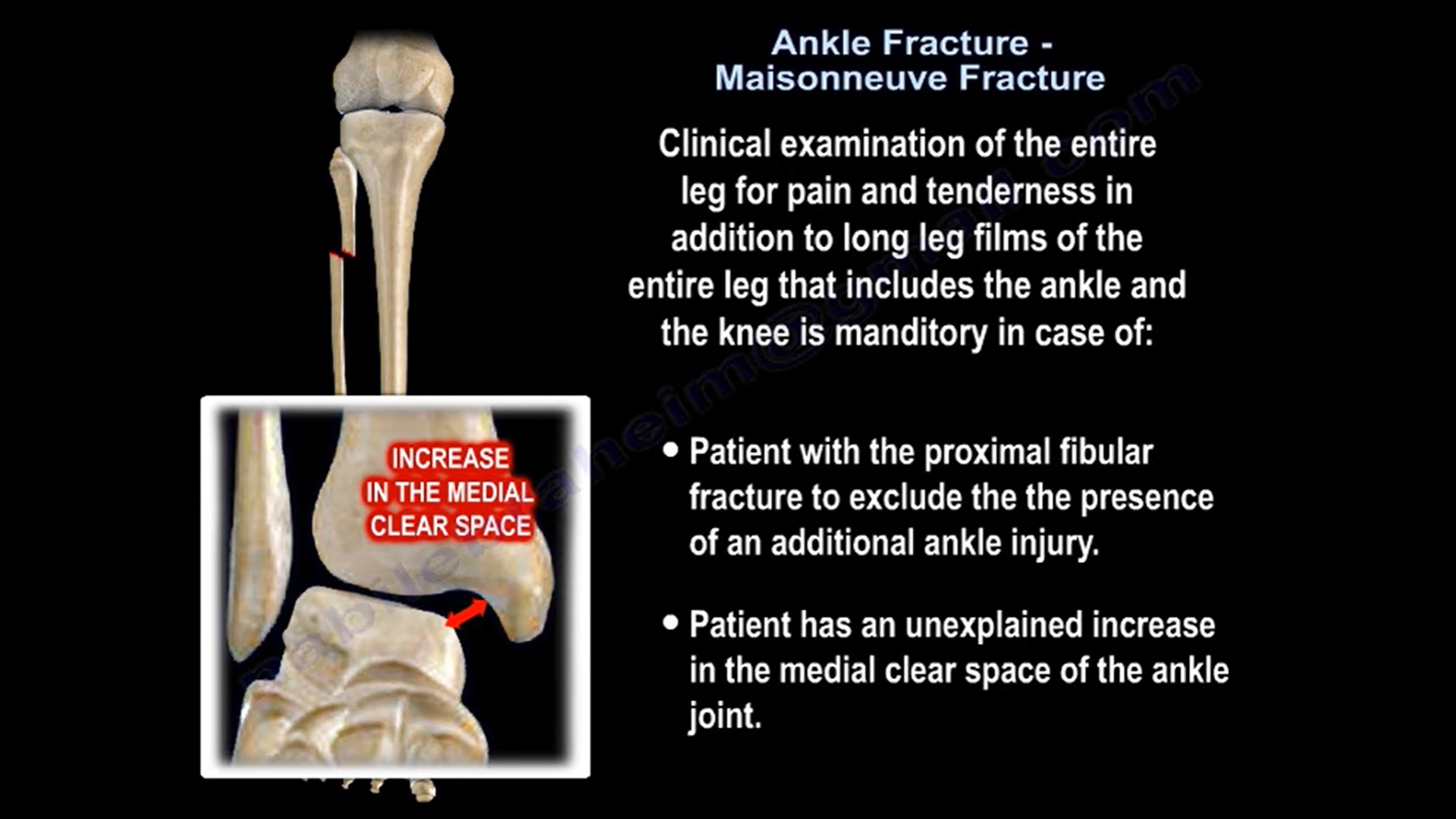
Long Leg Films are Mandatory in
1. Patients with a Proximal Fibular Fracture
To exclude an associated ankle syndesmotic injury.
2. Patients with Unexplained Medial Clear Space Widening
To identify a proximal fibular fracture.
Radiographic Signs of Syndesmotic Injury
Increased Medial Clear Space
Suggests injury to the deltoid ligament or syndesmosis.
Increased Tibiofibular Clear Space
Normally less than 5 mm.
A widened tibiofibular clear space indicates syndesmotic disruption.
Mechanism of Injury
Typically occurs due to:
- External rotation of the foot
- Usually combined with a pronation force
The rotational force travels:
- Through the ankle syndesmosis
- Along the interosseous membrane
- Exits proximally through a fracture of the proximal fibula
Structures Commonly Injured
Medial Side
- Deltoid ligament rupture
- Medial malleolus fracture
Syndesmosis
- Anterior inferior tibiofibular ligament (AITFL)
- Interosseous ligament
- Posterior inferior tibiofibular ligament (PITFL)
Posterior Side
- Posterior malleolus fracture
Lateral Side
- Proximal fibular fracture
Treatment
Principle
The key lesion is the syndesmotic injury.
Therefore treatment focuses on:
Reduction and Stable Fixation of the Syndesmosis
Usually performed using syndesmotic screws.
Management of Associated Injuries
Deltoid Ligament Tear
- Usually left alone
- Does not routinely require repair
Medial Malleolus Fracture
- Should be fixed
Proximal Fibular Fracture
- Usually does not require fixation
Syndesmotic Fixation
Because Maisonneuve fractures represent high energy syndesmotic injuries:
- Stable fixation is essential
- More syndesmotic screws may be required compared with routine ankle fractures
Postoperative Protocol
- Short leg splint or cast
- Strict non weight bearing for 6 to 8 weeks
- Progressive rehabilitation thereafter
Key Examination Pearls
- Always palpate the entire fibula in ankle injuries.
- A proximal fibular fracture should prompt examination of the ankle.
- Medial clear space widening without a lateral malleolar fracture should raise suspicion of a Maisonneuve injury.
- Obtain long leg radiographs whenever syndesmotic injury is suspected.
- The proximal fibular fracture is usually not the problem; the unstable syndesmosis is.
Take Home Message
Never diagnose a proximal fibular fracture without examining the ankle, and never diagnose a syndesmotic ankle injury without examining the proximal fibula. Missing a Maisonneuve fracture means missing an unstable ankle injury.

Leave a Reply