Courtesy Dr. Ram Chaddha, Dr Ashok Shyam, Ortho TV
Low Back Pain & Lumbar Disc Disease – Myths, Realities, and Management
Introduction
Low back pain is one of the most common conditions encountered in orthopedic practice. Nearly 80% of individuals experience low back pain at some point in life. Common causes include:
- Lumbar disc herniation
- Lumbar canal stenosis
- Degenerative disc disease
Modern management requires careful clinical judgment because imaging findings often do not correlate with symptoms.
Degenerative Disc Disease: Aging vs Pathology
Disc degeneration may represent:
- A normal physiological aging process
- A pathological condition causing symptoms
A major principle is that MRI severity does not necessarily correlate with clinical severity.
Examples include:
- Young patients with severe MRI degeneration but minimal symptoms
- Elderly patients with minimal MRI changes but significant disability
Imaging alone should never determine treatment decisions.
Juvenile Degenerative Disc Disease
Overview
Juvenile degenerative disc disease occurs in young individuals with early multilevel disc degeneration.
Possible contributing factors include:
- Genetic predisposition
Clinical Progression
Initially, symptoms may respond well to conservative treatment. However, progression can occur with development of:
- Radiculopathy
- Neurogenic claudication
- Neurological deficits
- Bladder dysfunction
- Sexual dysfunction
These later findings are considered important warning signs.
Red Flag Symptoms
Urgent evaluation is required when patients develop:
- Progressive neurological deficit
- Bladder dysfunction
- Bowel dysfunction
- Sexual dysfunction
- Severe or worsening radiculopathy
- Features of cauda equina syndrome
These symptoms may indicate significant neural compression requiring emergency assessment.
Principles Before Surgery
The Three Golden Rules
Successful spine care begins with:
- Counseling
- Counseling
- Counseling
Patient education and expectation management are critical.
Proper Surgical Decision-Making
Before considering surgery, the surgeon should answer:
- Why is surgery needed?
- How should surgery be performed?
- Which technique or implant should be used?
Modern practice often incorrectly focuses first on implants and technology rather than indications.
Treat the Patient, Not the MRI
Clinical-radiological mismatch is extremely common in spine disorders.
Management should be guided primarily by:
- Symptoms
- Functional limitation
- Neurological examination
MRI findings alone do not justify surgery.
Natural History of Lumbar Disc Herniation
Spontaneous Regression
Lumbar disc herniations frequently improve without surgery.
Reported outcomes include:
- Approximately 49% near-complete regression
- Approximately 39% partial regression
- Approximately 12% minimal or no regression
Symptoms often improve before MRI changes resolve.
Favorable Prognostic Factors
Better outcomes are associated with:
- Large disc herniations
- Extruded or sequestrated discs
- Improvement within 6 weeks
- Non-smokers
- Good general health
- Absence of psychosocial stressors
Unfavorable Prognostic Factors
Poorer prognosis is associated with:
- Positive crossed straight leg raise
- Persistent symptoms beyond 6 weeks
- Progressive neurological deficit
- Contained disc herniation
- Psychological factors
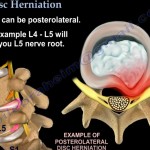
Pathophysiology of Disc Herniation
Disc herniation occurs due to:
- Annular tear
- Extrusion of nucleus pulposus
Symptoms arise from two major mechanisms:
- Mechanical nerve compression
- Chemical inflammatory irritation
Both contribute to pain and neurological symptoms.
Conservative Management
First-Line Treatment
Most patients improve with non-operative management.
Treatment options include:
- NSAIDs
- Neuropathic pain medications
- Physiotherapy
- Activity modification
- Patient education
Evidence-Based Points
Bed Rest
Bed rest should be limited to:
- 1–3 days only
Prolonged bed rest is not beneficial.
Traction
Systematic reviews show:
- No proven benefit of lumbar traction
Emerging Non-Surgical Treatments
Newer treatment strategies include:
- Chemonucleolysis
- Intradiscal ethanol gel injection
- Platelet-rich plasma (PRP)
- Stem cell therapies
- Monoclonal antibodies targeting inflammation
- Structured rehabilitation programs (“back school”)
Many remain investigational or evolving.
Indications for Surgery
Surgery should be reserved for select situations, including:
- Cauda equina syndrome
- Progressive motor deficit
- Foot drop
- Persistent severe radicular pain despite conservative treatment
- Significant functional impairment with clinical-radiological correlation
Surgical Principles
Microdiscectomy
Microdiscectomy is the standard surgical treatment for symptomatic lumbar disc herniation.
Key Surgical Principle
The primary goal is:
- Nerve root decompression
Not aggressive disc removal.
Technical Principles
Recommended steps include:
- Foraminotomy
- Removal of herniated fragment
Aggressive disc curettage should be avoided because it may:
- Increase risk of discitis
- Accelerate degeneration
Fusion vs Non-Fusion Surgery
Fusion Indications
Fusion may be indicated in:
- Instability
- Recurrent disc disease with back pain
- Degenerative spondylolisthesis
Non-Fusion Preferred
Non-fusion surgery is preferred when:
- Radiculopathy is isolated
- No instability is present
Lumbar Canal Stenosis
Clinical Features
Lumbar stenosis commonly presents with:
- Neurogenic claudication
- Leg heaviness
- Walking intolerance
Symptoms improve with:
- Sitting
- Forward bending
Surgical Indications
Surgery is considered for:
- Disabling neurogenic claudication
- Severe stenosis
- Cauda equina syndrome
Surgical Considerations
Decompression Alone
Used for:
- Central stenosis
- Lateral recess stenosis
Add Fusion If
- Instability exists
- Extensive facetectomy is required
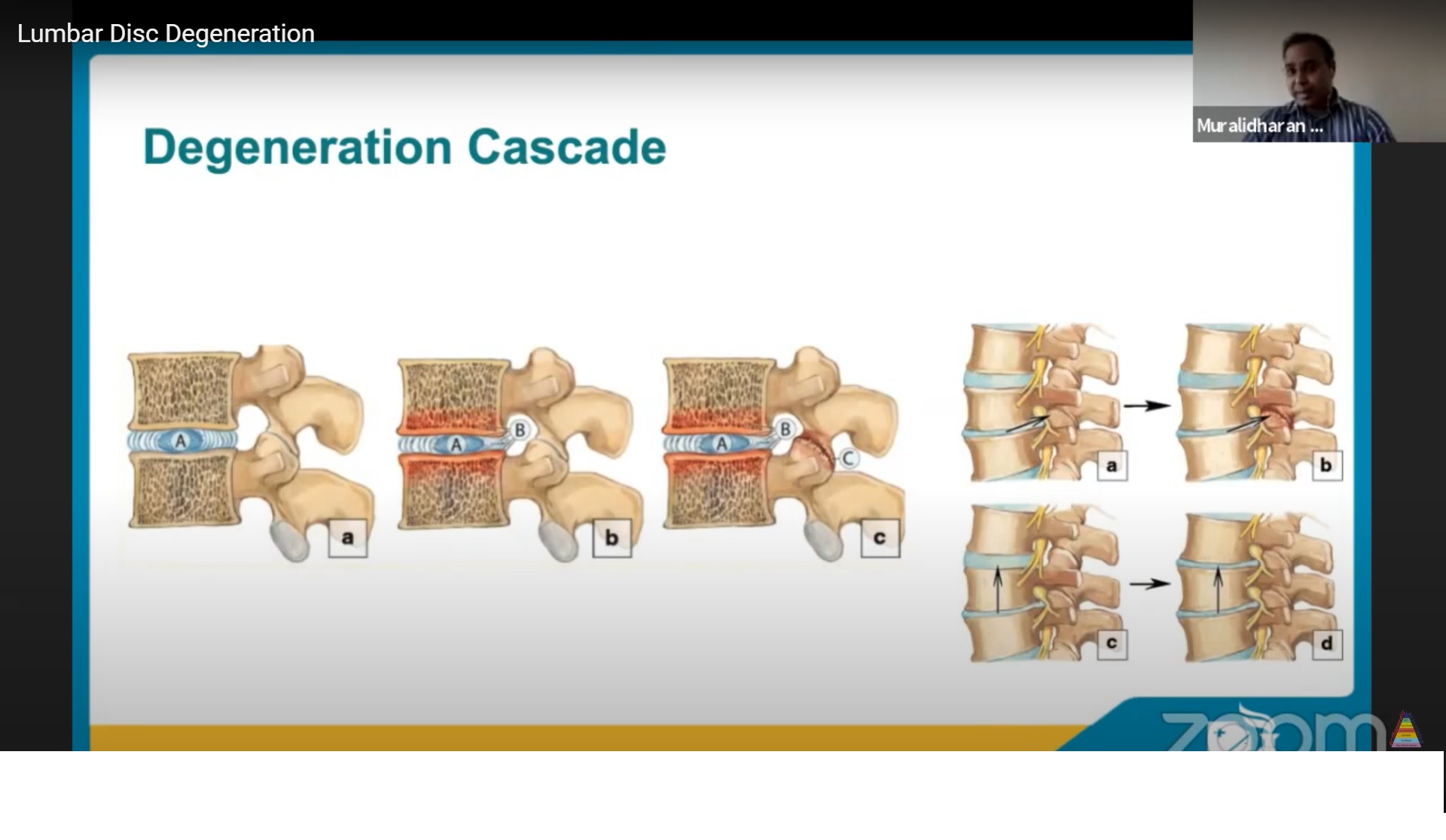
Kirkaldy-Willis Degenerative Cascade
The degenerative process progresses through three phases:
- Dysfunction phase
- Instability phase
- Stabilization phase
Many patients improve if managed conservatively through the instability phase.
Revision Surgery Principles
Most recurrent disc herniations require:
- Repeat decompression only
A smaller group may require:
- Instrumentation
- Fusion surgery
Clinical Decision-Making Pearls
Important practical principles include:
- Symptoms greater than signs often favor conservative treatment
- Signs greater than symptoms may justify surgery
- Avoid overtreatment in elderly patients
- Treat osteoporosis before major spinal surgery
Technological Considerations
Modern spine surgery increasingly uses:
- Minimally invasive techniques
- Robotics
- Biologics
Gene therapy may become important in the future.
However, technology should never replace sound clinical judgment.
Key Surgical Philosophy
Spine surgery should begin with:
- Purpose
- Patient selection
- Clinical reasoning
rather than:
- Technology-driven decisions
- Implant-driven marketing
Key Take-Home Messages
- Most lumbar disc herniations improve without surgery.
- Large herniations often regress spontaneously.
- MRI findings alone do not indicate surgery.
- Counseling is critical to successful outcomes.
- Surgery should be reserved for carefully selected patients.
- Good judgment is more important than aggressive intervention.
- Experience in spine surgery develops through careful learning and complication management.
Leave a Reply