Courtesy: Ioannis Stavrakakis MD, Crete, Greece
Introduction
A Lisfranc injury involves the tarsometatarsal (TMT) joint complex of the midfoot. These injuries range from subtle ligament sprains to severe fracture dislocations and are frequently missed, leading to chronic pain, instability, and post traumatic arthritis.
The injury is named after Jacques Lisfranc de St. Martin, who originally described amputations through the tarsometatarsal joint level.
Anatomy
Bony Anatomy
The midfoot consists of:
- Three cuneiform bones
- Cuboid
- Five metatarsal bases
The key stabilizing feature is the second metatarsal base, which is recessed between the medial and lateral cuneiforms.
Keystone Concept
The second metatarsal functions as the “keystone” of the midfoot arch, similar to the central stone in a Roman arch.
This unique anatomy provides substantial stability to the tarsometatarsal joint complex.
Ligamentous Anatomy
The Lisfranc ligament complex consists of:
Dorsal Ligament
- Weakest component
Interosseous Lisfranc Ligament
- Strongest component
- Thickest ligament
- Extends from the medial cuneiform to the base of the second metatarsal
- Provides greatest resistance to displacement
Plantar Ligament
- Strong secondary stabilizer
Neurovascular Anatomy
The neurovascular bundle:
- Lies lateral to the extensor hallucis longus tendon
- Runs beneath the muscle belly of extensor hallucis longus
- Must be protected during surgical exposure
Epidemiology
- Approximately 0.2% of all fractures
- Incidence likely underestimated because many injuries are missed
- Men affected 2 to 4 times more commonly than women
- Common in athletes and young adults
- Most injuries are closed
Mechanism of Injury
Direct Injury
Examples include:
- Heavy object falling onto the dorsum of the foot
- Crush injuries
- Motor vehicle accidents
Indirect Injury (Most Common)
Occurs when:
- Foot is plantarflexed
- Forefoot undergoes rotational force
This mechanism places significant stress across the tarsometatarsal joint complex and may disrupt the Lisfranc ligament.
Clinical Features
Symptoms
- Midfoot pain
- Difficulty walking
- Inability to bear weight
- Swelling
Examination Findings
Important Signs
- Midfoot tenderness
- Swelling over TMT joints
- Pain with forefoot twisting
- Pain during heel raise
Plantar Ecchymosis Sign
A plantar bruise is highly suggestive of a Lisfranc injury and may appear several days after trauma.
Neurovascular Assessment
Always assess:
- Dorsalis pedis pulse
- Sensation
- Signs of compartment syndrome
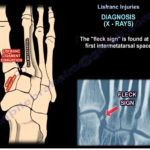
Imaging
Plain Radiographs
Essential views include:
AP View
Assess alignment of:
- Medial border of second metatarsal
- Medial border of intermediate cuneiform
Oblique View
Evaluates:
- Third and fourth TMT joints
- Lateral column alignment
True Lateral View
Assesses:
- Dorsal displacement
- Sagittal plane instability
Weight Bearing Radiographs
Often the most useful investigation for subtle injuries.
Advantages
- Demonstrates instability
- Reveals widening between first and second metatarsals
- Allows comparison with the opposite foot
Bilateral weight bearing radiographs are particularly valuable.
CT Scan
Indications
- Diagnostic uncertainty
- Fracture assessment
- Surgical planning
Advantages
- Identifies occult fractures
- Demonstrates joint incongruity
- Defines fracture patterns
Weight Bearing CT
Provides:
- Functional assessment under load
- Improved detection of subtle instability
Limitation:
- Limited availability
MRI
Role
Not routinely required.
Useful when:
- Diagnosis remains uncertain
- Assessment of ligament integrity is needed
- Stable injuries require confirmation
Classification
Myerson Classification
Type A (Homolateral)
- Entire forefoot displaced in one direction
- Medially or laterally
Type B (Partial Incongruity)
- Partial displacement
- Medial or middle column involvement
Type C (Divergent)
- Medial and lateral columns separate
- Most severe pattern
Nunley Classification
Used primarily for subtle athletic injuries.
Grade 1
- Ligament sprain
- No diastasis
Grade 2
- Partial ligament disruption
- 2 to 5 mm separation between first and second metatarsals
Grade 3
- Complete ligament disruption
- Greater than 5 mm separation
Treatment
Stable Injuries
Criteria
- No diastasis
- No instability on weight bearing radiographs
Treatment
- Non weight bearing cast or boot for 6 weeks
- Followed by walking boot for approximately 4 weeks
- Gradual rehabilitation
Unstable Injuries
Criteria
- Widening between first and second metatarsals
- Displacement on stress or weight bearing imaging
Treatment
Surgical stabilization is recommended.
Options include:
- Open reduction and internal fixation (ORIF)
- Primary arthrodesis (fusion)
Surgical Management
ORIF
Traditional approach using:
- Transarticular screws
- Bridge plates
- Combination constructs
Advantages
- Preserves joints
- Allows restoration of anatomy
Primary Fusion
Fusion of unstable joints, particularly:
- First TMT joint
- Medial column injuries
Evidence
Many studies demonstrate:
- Similar outcomes compared with ORIF
- Slight trend toward improved functional scores in some series
However, differences are often not clinically significant.
Screw Fixation vs Bridge Plating
Bridge Plate Advantages
- Better reduction quality
- Slightly improved functional outcomes in some studies
Biomechanics
Both techniques provide comparable stability.
Percutaneous Fixation
Indications
Selected injuries with:
- Minimal displacement
- Reducible Type B patterns
Advantages
- Less soft tissue dissection
- Reduced surgical morbidity
Success depends on achieving an anatomical reduction.
Surgical Principles
Stress Fluoroscopy
Perform before fixation to identify:
- Unstable rays
- Additional ligament injuries
Common Fixation Strategy
May include:
Home Run Screw
Placed from:
- Medial cuneiform
- Into the second metatarsal base
Restores Lisfranc stability.
Additional Procedures
- First TMT fusion if unstable
- Bridge plating of second and third TMT joints
Timing of Surgery
Definitive Fixation
Usually delayed:
- 10 to 15 days after injury
- Allows swelling to subside
Severe Dislocations
If marked displacement exists:
Initial Management
- Closed reduction
- Temporary K wire fixation
- External fixation if required
Definitive Surgery
Performed once soft tissues recover.
Implant Removal
Current Evidence
Routine implant removal is not always necessary.
Screw Fixation
Often removed around 6 months.
Plates
Usually retained unless symptomatic.
Functional outcomes appear similar whether implants are removed or retained.
Postoperative Protocol
First 6 Weeks
- Posterior splint or cast
- Strict non weight bearing
Following 4 Weeks
- Partial weight bearing in walking boot
Rehabilitation
- Progressive return to full weight bearing
- Strengthening and gait training
Associated Injuries
Always assess for:
- Metatarsal fractures
- Cuneiform fractures
- Cuboid injuries
- Additional midfoot instability
- Other tarsal injuries
Take Home Messages
- The second metatarsal is the keystone of the Lisfranc joint complex.
- Plantar ecchymosis is a highly important clinical sign.
- Weight bearing radiographs are essential when a Lisfranc injury is suspected.
- CT scanning is extremely useful for detecting occult fractures and surgical planning.
- Stable injuries can be managed nonoperatively.
- Unstable injuries generally require surgical stabilization.
- Anatomical reduction is the most important predictor of a successful outcome.
- The debate between ORIF and primary fusion continues, but both can provide excellent results when reduction is achieved accurately.


Leave a Reply