Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Sciatic Nerve Lesions and Clinical Relevance
Introduction
The sciatic nerve is the largest nerve in the human body and is of major clinical importance in orthopaedics, trauma, spine surgery, and hip surgery.
Sciatic nerve pathology may result from:
- Trauma
- Compression
- Surgical injury
- Spinal disorders
- Extra-spinal causes such as piriformis syndrome
Understanding its anatomy and clinical presentation is essential for accurate diagnosis and management.
Anatomy of the Sciatic Nerve
Formation
The sciatic nerve is formed from:
- L4
- L5
- S1
- S2
- S3 nerve roots
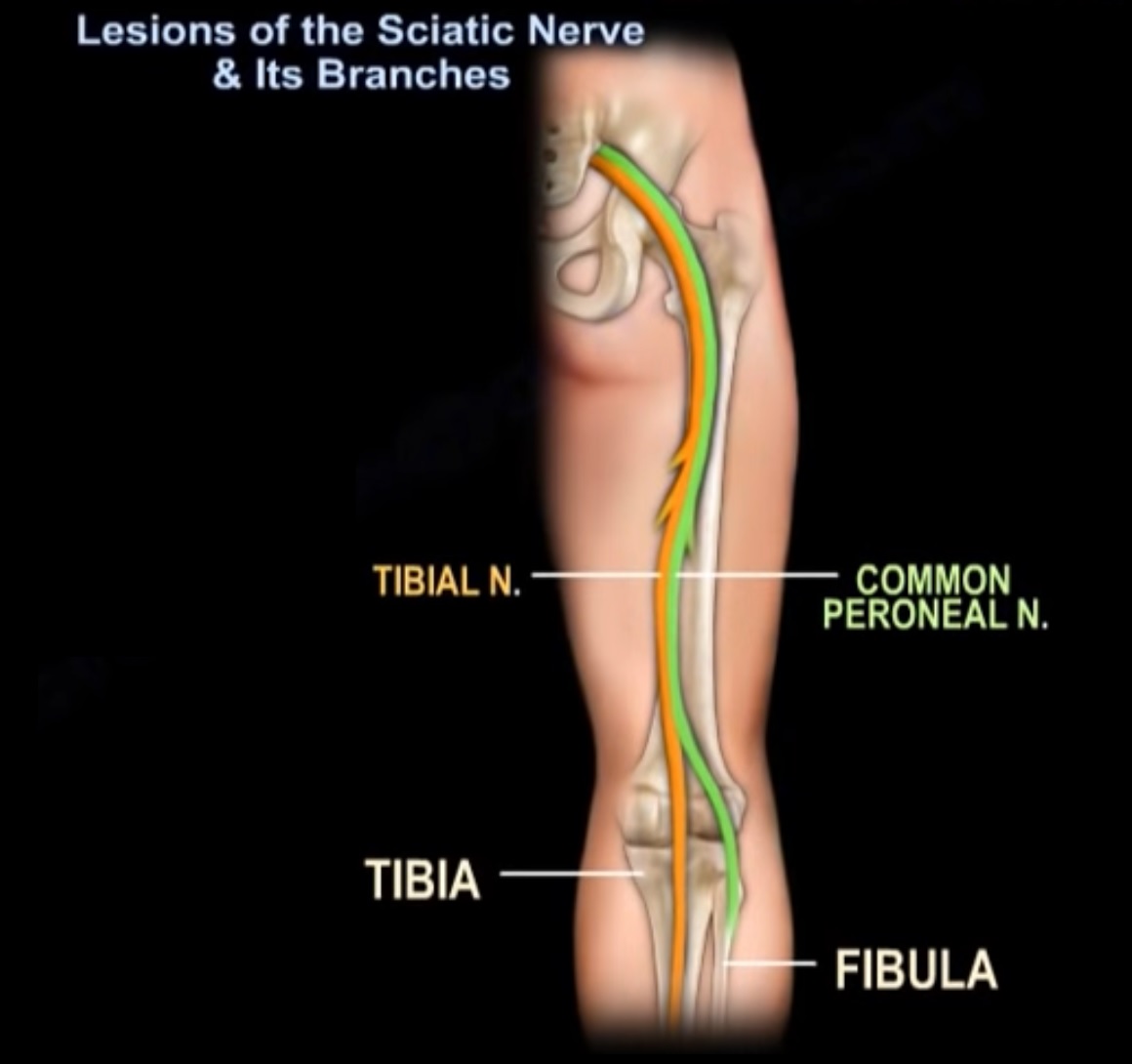
It contains two major components:
- Tibial nerve
- Common peroneal (fibular) nerve
Course of the Sciatic Nerve
The sciatic nerve follows this pathway:
- Originates from the lumbosacral plexus
- Exits the pelvis through the greater sciatic foramen
- Usually passes below the piriformis muscle
- Travels deep to the gluteus maximus
- Runs along the posterior thigh
- Divides into tibial and common peroneal nerves in the distal thigh
Anatomical Variations
In approximately 10% of individuals:
- Division of the sciatic nerve occurs within the pelvis
These variations are important during hip surgery and in piriformis syndrome.
Important Anatomical Relations
The sciatic nerve lies:
- Posterior to the obturator internus and quadratus femoris
- Close to the ischium
Because of this relationship, it is vulnerable in:
- Posterior hip dislocations
- Acetabular fractures
- Posterior surgical approaches to the hip
Causes of Sciatic Nerve Injury
Traumatic Causes
Common traumatic causes include:
- Posterior hip dislocation
- Acetabular fractures
- Pelvic fractures
- Sacroiliac joint displacement
Pelvic injuries may also involve the lumbosacral plexus.
Iatrogenic Causes
Sciatic nerve injury may occur during surgery due to:
- Posterior hip approaches
- Retractor misplacement
- Excessive limb lengthening during total hip arthroplasty
- Acetabular screw misplacement
Most Vulnerable Division
The common peroneal division is affected more frequently because:
- It contains fewer fascicles
- It is more fixed and less elastic
This explains why foot drop is common in sciatic nerve injury.
Clinical Features of Sciatic Nerve Injury
Motor Deficits
Typical findings include:
- Foot drop
- Weak ankle dorsiflexion
- Weak toe extension
Severe injuries may also affect plantarflexion.
Sensory Loss
Sensory deficits commonly involve:
- Lateral aspect of the leg
- Dorsum of the foot
Gait Abnormality
Patients may develop:
- High-stepping gait due to foot drop
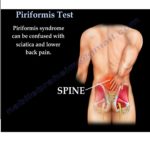
Piriformis Syndrome
Definition
Piriformis syndrome is an extra-spinal cause of sciatica caused by compression of the sciatic nerve by the piriformis muscle.
Clinical Importance
Piriformis syndrome may closely mimic:
- Lumbar disc herniation
- Radiculopathy
It should be considered when:
- MRI of the lumbar spine is normal
- Symptoms persist despite spinal treatment
Mechanism
The piriformis muscle compresses or irritates the sciatic nerve, particularly during:
- Hip flexion
- Adduction
- Internal rotation
Clinical Features of Piriformis Syndrome
Patients may present with:
- Buttock pain
- Sciatic-type leg pain
- Tenderness near the sciatic notch
- Pain worsened by sitting
- Pain aggravated by stretching the piriformis muscle
Clinical Examination
Straight Leg Raise (Lasegue Test)
Technique
- Hip flexed
- Knee extended
Positive Test
Reproduction of sciatic pain suggests nerve irritation.
FAIR Test
FAIR stands for:
- Flexion
- Adduction
- Internal Rotation
Mechanism
This position stretches the piriformis muscle and may compress the sciatic nerve.
Positive Test
Reproduction of buttock or sciatic pain indicates piriformis syndrome.
Important Clinical Distinction
- FAIR test ? suggests piriformis syndrome
- FABER test ? suggests sacroiliac or hip pathology
Diagnosis
Diagnosis of Exclusion
Piriformis syndrome should only be diagnosed after excluding spinal causes such as:
- Lumbar disc herniation
- Foraminal stenosis
- Lumbar radiculopathy
MRI of the lumbar spine is often required.
Surgical Precautions
Posterior Hip Approach
To minimize sciatic nerve stretch during surgery:
- Hip should be kept extended
- Knee should be flexed
This reduces tension on the sciatic nerve.
Key Clinical Pearls
- The sciatic nerve usually passes below the piriformis muscle.
- Posterior hip dislocation is a common traumatic cause of sciatic nerve injury.
- The common peroneal division is most vulnerable.
- Foot drop is the classic presentation.
- Piriformis syndrome is an important extra-spinal cause of sciatica.
- Not all sciatica is caused by lumbar disc prolapse.
- Always correlate clinical findings with imaging.
Final Take-Home Message
The sciatic nerve is the principal nerve of the lower limb and is vulnerable to injury in trauma, spinal disorders, and hip surgery.
Sciatic nerve lesions commonly present with:
- Foot drop
- Sensory loss
- Sciatic pain
Piriformis syndrome is an important differential diagnosis in patients with sciatica and normal lumbar imaging.
Careful clinical examination and appropriate imaging are essential for accurate diagnosis and treatment.

Leave a Reply