Courtesy: Dr Ranawat, Ashok Shyam TV, Ortho
Evolution in Meniscus Root Management
-
Meniscus root repair represents a major advancement in knee preservation surgery.
-
The medial root has transformed arthritis prevention strategies.
-
The lateral root is increasingly recognized as critical for knee stability, particularly in anterior cruciate ligament–deficient knees.
-
Modern sports medicine now emphasizes identifying and repairing both medial and lateral root tears when indicated.
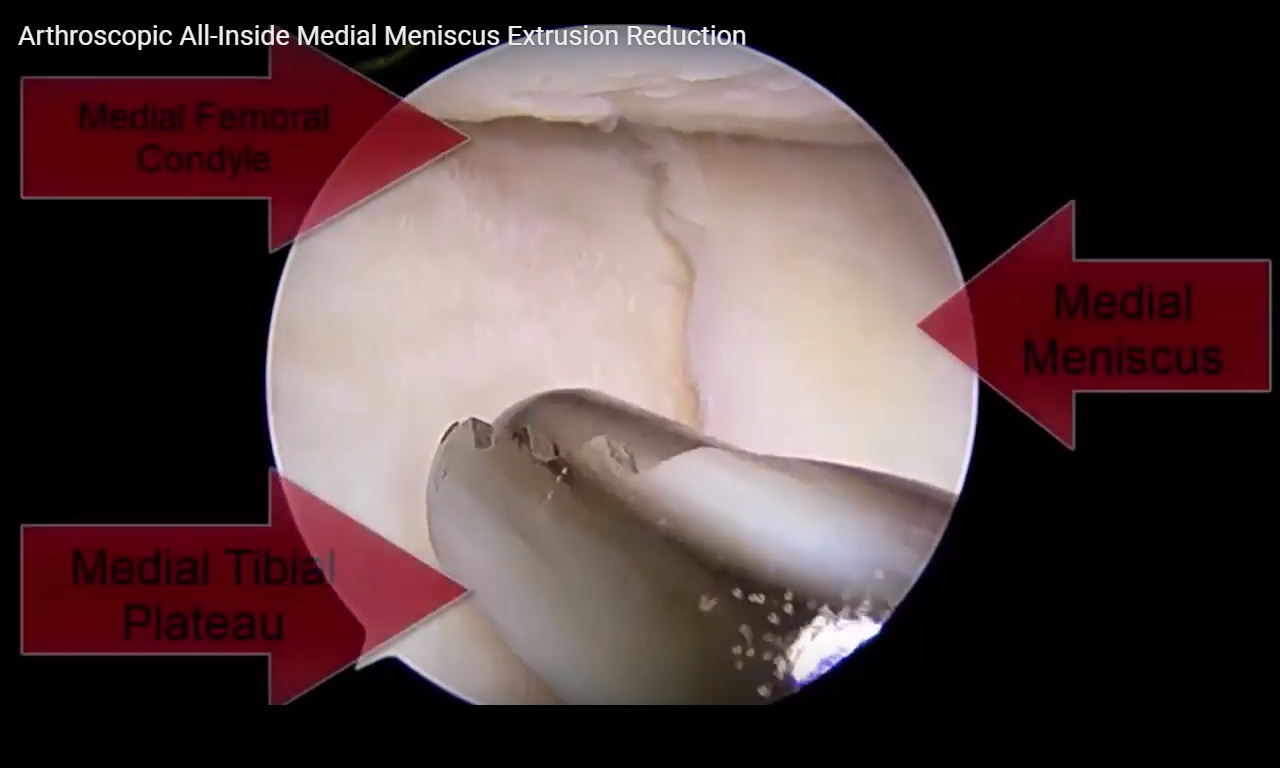
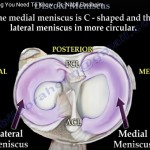
Anatomic Relationships
Understanding root anatomy is essential:
-
Medial meniscus root
-
Closely related to the posterior cruciate ligament.
-
Arthroscopically and anatomically “married” to the posterior cruciate ligament.
-
-
Lateral meniscus root
-
Closely related to the posterolateral bundle of the anterior cruciate ligament.
-
Critical during primary and especially revision anterior cruciate ligament reconstruction.
-
Anatomic awareness prevents iatrogenic injury during tunnel drilling and improves diagnostic vigilance.
Medial vs Lateral Root: Different Clinical Roles
Medial Root
-
Strongly associated with contact mechanics.
-
Considered disease-modifying surgery.
-
Repair may reduce progression to osteoarthritis.
-
Approximately 60 to 70 percent success in altering disease course.
Lateral Root
-
More strongly associated with stability.
-
Particularly important in rotational control.
-
Cutting the lateral meniscus increases internal rotation in mid-flexion.
-
Considered the most important lateral stabilizer of the knee.
Biomechanical Significance of the Lateral Root
-
Contributes significantly to rotational stability.
-
Plays a major role in high-grade pivot shift.
-
Secondary stabilizer in anterior cruciate ligament–deficient knees.
-
Important in revision anterior cruciate ligament failure.
Emerging evidence suggests:
-
Both primary and secondary effects on contact pressures.
-
However, stability remains the dominant clinical issue.
Missed Lateral Root Tears
-
Often underdiagnosed.
-
More difficult to detect than medial root tears.
Incidence:
-
Approximately 7 percent in primary anterior cruciate ligament reconstruction.
-
Up to 40 percent in revision anterior cruciate ligament surgery.
High suspicion is essential in:
-
Revision cases.
-
High-grade pivot shift.
-
Persistent instability despite technically adequate anterior cruciate ligament reconstruction.
Clinical Clue in Revision Anterior Cruciate Ligament Surgery
Typical scenario:
-
Tunnels acceptable.
-
Graft choice appropriate.
-
Alignment normal.
-
Yet graft failure occurs.
Key finding:
-
Previously missed lateral meniscus root tear.
Addressing the root tear may prevent repeated failure.
Diagnosis Pearls
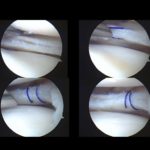
Arthroscopic Evaluation
-
Lateral root tears are subtle.
-
Must:
-
Carefully inspect.
-
Probe thoroughly.
-
Avoid being misled by meniscofemoral ligaments that may provide temporary stabilization.
-
Magnetic Resonance Imaging
-
Medial root tear: relatively straightforward diagnosis.
-
Lateral root tear: frequently missed.
-
“Ghost sign” may be present but not always.
High index of suspicion is mandatory in revision anterior cruciate ligament surgery.
Surgical Pearls for Lateral Root Repair
1. Exposure is Critical
-
Use figure-four positioning.
-
Optimize lateral compartment visualization.
-
Avoid excessive lateral compartment constraint.
2. Tight Lateral Compartment
-
If compartment is tight:
-
Avoid over-constraint procedures such as lateral extra-articular tenodesis.
-
Prioritize root repair.
-
3. Tunnel Creation
-
Use root-specific guides when possible.
-
Guides that wrap around tibial spines improve accuracy.
-
Decorticate the root footprint to enhance healing.
-
Soft tissue–to–bone healing is superior to soft tissue–to–soft tissue healing.
4. Independent Tunnel Strategy
-
Create a separate tibial tunnel for the lateral root.
-
Ensure it is sufficiently medial to avoid convergence with anterior cruciate ligament tunnel.
-
In small knees, space is limited and precision is critical.
Technical safeguard:
-
Insert arthroscope into tibial tunnel after drilling.
-
Confirm independence from anterior cruciate ligament tunnel.
-
Only pass sutures after confirmation.
Fixation Principles
-
Use strong suture configurations such as locking or luggage tag stitches.
-
Ensure secure fixation into decorticated bone.
-
Avoid tunnel collision.
-
Confirm anatomic positioning before final fixation.
Outcomes and Emerging Evidence
Current trends suggest:
-
Ignoring lateral root tears may:
-
Increase anterior cruciate ligament graft failure.
-
Increase instability.
-
Possibly increase long-term degenerative changes.
-
-
Repair may:
-
Improve stability.
-
Reduce rerupture risk.
-
Improve pivot control.
-
Large, long-term studies are still emerging.
Case Example: Recurrent ACL Failure
Young patient with:
-
Primary anterior cruciate ligament reconstruction.
-
Revision reconstruction.
-
Persistent high-grade pivot shift.
-
Acceptable tunnels.
-
Acceptable alignment.
-
Normal collateral stability.
Key finding:
-
Missed lateral meniscus root tear.
Management:
-
Revision anterior cruciate ligament reconstruction.
-
Lateral meniscus root repair.
-
No lateral extra-articular tenodesis due to tight lateral compartment.
Key Surgical Philosophy
High-grade pivot shift indicates:
-
Loss of secondary stabilizers.
Repeated anterior cruciate ligament reconstruction alone without addressing secondary pathology is insufficient.
Practical Recommendations
-
Always inspect the lateral root carefully during anterior cruciate ligament surgery.
-
Maintain high suspicion in revision cases.
-
Repair lateral root tears when identified.
-
Consider routine fixation during revision anterior cruciate ligament reconstruction.
-
Many surgeons now advocate repairing lateral root tears even during primary anterior cruciate ligament reconstruction when present.
Conclusion
-
Medial root repair is primarily disease-modifying.
-
Lateral root repair is primarily stability-restoring.
-
Lateral meniscus is the most important lateral stabilizer of the knee.
-
Missed lateral root tears are a common cause of anterior cruciate ligament graft failure.
-
Careful inspection, independent tunnel creation, and secure fixation are essential.
-
In revision anterior cruciate ligament surgery, always evaluate and address the lateral meniscus root.
Leave a Reply