Courtesy: Dr S Macdonald, Ashok Shyam TV, Ortho
Significant extra-articular deformities are relatively uncommon in many Western practices but may be more frequently encountered in post-traumatic populations. Common causes include:
-
Malunited fractures
-
Prior osteotomies
-
Metabolic bone disease (e.g., Paget’s disease)
The challenge is achieving proper limb alignment without compromising ligament stability.
Three Treatment Options
When facing extra-articular deformity in a patient requiring TKA, there are three main strategies:
-
Intra-articular bone resection + soft tissue balancing
-
Simultaneous corrective osteotomy + TKA
-
Staged corrective osteotomy followed by delayed TKA
The decision depends on deformity magnitude, location, and impact on ligament attachments.
Alignment Principles Remain the Same
Regardless of deformity:
-
Distal femoral cut ? 90° to mechanical axis
-
Tibial cut ? 90° to tibial mechanical axis
-
Goal ? restore neutral mechanical alignment
Standard distal femoral valgus angle (5–7° to anatomical axis) still applies.
Option 1: Intra-Articular Correction
When Is It Feasible?
-
Femoral varus/valgus deformity < 20°
-
Tibial deformity up to ~30°
-
Flexion/extension deformity up to ~25°
-
Deformity not compromising collateral ligament origin/insertion
Key Rule
If planned bone cuts do NOT violate the:
-
Femoral origin of collateral ligaments
-
Tibial insertion of collateral ligaments
? Correction can be achieved through intra-articular resection.
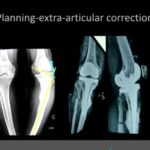
Preoperative Planning
-
Draw mechanical axis (hip ? knee ? ankle).
-
Map resection lines.
-
Determine whether ligament attachments will remain intact.
Technical Consideration
Intramedullary guides may not be usable.
Alternative strategy:
-
Extramedullary referencing.
-
Fluoroscopy-assisted localization of femoral head center.
-
Surface landmark referencing.
Posterior stabilized (PS) design is often preferred to simplify balancing.
Advantages
-
Single procedure.
-
Avoids osteotomy healing complications.
-
Reliable when deformity is moderate.
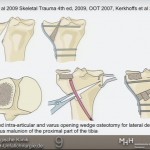
Option 2: Simultaneous Osteotomy + TKA
Indications
-
Deformity > 20°–30°
-
Deformity close to joint line
-
Intra-articular correction would destabilize knee
-
Ligament attachments would be compromised
Key Technical Principle
-
Perform corrective osteotomy.
-
Use stemmed components to bypass osteotomy site.
-
Restore alignment and protect fixation.
Advantages
-
One-stage correction.
-
Immediate mechanical realignment.
Risks
-
Nonunion
-
Malunion
-
Delayed healing
-
Increased surgical complexity
Option 3: Staged Osteotomy Then TKA
Increasingly preferred when:
-
Deformity is remote from joint.
-
Severe angular deformity.
-
Custom long stems would be required.
-
Risk of nonunion is high.
Approach
-
Correct deformity first.
-
Allow complete union.
-
Perform standard TKA later.
Why Consider Staging?
Simultaneous correction may:
-
Increase nonunion rates.
-
Increase fixation complexity.
-
Compromise long-term results.
Staged approach may provide:
-
More predictable bone healing.
-
Simpler TKA.
-
Better long-term mechanical stability.
Key Decision Factors
1?? Magnitude of Deformity
Greater deformity ? more likely to require osteotomy.
2?? Distance from Joint Line
Closer to joint ? more impact on ligament balancing.
3?? Ligament Integrity
If bone cuts would violate collateral ligaments ? osteotomy required.
4?? Rotational Deformity
Often underestimated.
CT scan may be required to assess internal/external rotation.
Practical Thresholds (General Guidelines)
| Location | Intra-articular Correction Possible |
|---|---|
| Femur | < 20° varus/valgus |
| Tibia | Up to 30° |
| Sagittal deformity | ~25° |
| Severe supracondylar deformity | Often needs osteotomy |
These are guidelines, not absolute rules.
Common Pitfalls
-
Ignoring rotational deformity.
-
Underestimating ligament compromise.
-
Attempting simultaneous osteotomy in very severe deformity.
-
Not bypassing osteotomy with adequate stem length.
Final Algorithm
-
Define deformity (long-leg films ± CT).
-
Draw mechanical axis.
-
Map resection lines.
-
Assess ligament attachment preservation.
-
Choose:
-
Intra-articular correction (if safe).
-
Simultaneous osteotomy + stemmed TKA.
-
Staged osteotomy followed by TKA.
-
Take-Home Messages
-
Most moderate deformities can be managed intra-articularly.
-
Severe deformities near the joint often require osteotomy.
-
Remote deformities may be better treated in stages.
-
Stemmed implants are essential when osteotomy performed.
-
Alignment goals remain unchanged despite deformity.

Leave a Reply