Courtesy Dr Greg Bain, Dr Ashok Shyam, Ortho TV
Kienböck Disease (Avascular Necrosis of the Lunate)
Overview
Kienböck disease is a condition characterized by avascular necrosis of the lunate, leading to:
- Progressive lunate collapse
- Carpal instability
- Secondary degenerative arthritis of the wrist
It is a multifactorial disease involving mechanical, vascular, and structural factors
Pathophysiology
Multifactorial Mechanism
The disease results from a combination of:
- Lunate microstructure vulnerability
- Venous drainage abnormalities
- Repetitive mechanical stress
- Intraosseous (bone) compartment syndrome
- Altered wrist biomechanics
Key Concept
- Venous outflow obstruction + mechanical overload
More important than arterial insufficiency alone
Risk Factors and Predisposing Anatomy
Lunate Morphology
- Type I lunate:
- Single distal articulation (with capitate)
- Less stable
- Smaller lunate
- Uncovered lunate:
- Reduced support from distal radius
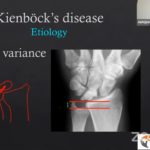
Ulnar Variance
- Negative ulnar variance:
- Ulna shorter than radius
- Increased load on lunate
Biomechanics of Lunate Loading
- Radial deviation — volar ligaments tighten
- Creates cantilever force on lunate
Result
- Increased load on proximal lunate
- Leads to:
- Subchondral microfractures
- Progressive collapse
Microstructure of the Lunate
Normal Structure
- Trabecular struts connect:
- Proximal and distal subchondral plates
- Transmit compressive forces
Pathological Changes
- Trabecular failure
- Microfractures
- Collapse
Important Note
- Proximal subchondral plate is very thin (~0.1 mm)
Highly vulnerable to stress
Mechanism of Lunate Fracture
Nutcracker Effect
- Lunate compressed between:
- Capitate
- Radius
Outcome
- Coronal plane fractures
- Fragment propagation toward triquetrum
Vascular Considerations
Arterial Supply
- Variable:
- Dorsal
- Volar
- Combined supply
Limitation
- Arterial variation alone does not explain disease
Venous Drainage (Key Concept)
Features
- Subchondral venous plexus
- Parallel venous channels
Pathology
- Fracture or collapse — venous obstruction
- Leads to:
- Venous congestion
- Ischemia
- Osteonecrosis
Compartment Syndrome of Bone
Mechanism
- Lunate behaves as a closed compartment
Pressure Changes
- Normal:
- Arterial ~60 mmHg
- Venous ~5–10 mmHg
In Disease
- Intraosseous pressure — (up to 150 mmHg)
Outcome
- Ischemia
- Bone necrosis
Cellular Changes
- Fat cell hypertrophy
- Marrow edema
- Increased intraosseous pressure
Further worsens venous outflow
Revascularization Potential
Younger Patients
- Better healing potential
- New bone formation from:
- Dorsal cortex
- Volar cortex
Clinical Insight
- Younger age — better prognosis
Assessment of Lunate Vascularity
MRI with Gadolinium
- Detects perfusion
Interpretation
- Enhancement — viable bone
- No enhancement — necrosis
Helps guide surgical planning
Articular Cartilage Changes
Progression
- Cartilage ulceration
- Subchondral sclerosis
- Surface irregularity
- Bone exposure
Arthroscopy Role
- Assess functional status of articulation
Functional vs Non-Functional Articulation
Functional
- Smooth surface
- Intact cartilage
- Glistening appearance
Non-Functional
- Rough surface
- Cartilage loss
- Exposed bone
Classification Systems
1. Lichtman Classification (Most Used)
Stage I
- Normal X-ray
- MRI: edema
Stage II
- Lunate sclerosis
- No collapse
Stage IIIA
- Lunate collapse
- Normal carpal alignment
Stage IIIB
- Collapse + DISI deformity
Stage IV
- Degenerative arthritis
2. Articular Surface Classification
- Based on cartilage integrity
- Helps guide motion-preserving surgery
3. Vascular Classification
- Based on MRI perfusion
- Determines bone viability
Treatment Principles
Factors Influencing Treatment
- Age
- Lunate integrity
- Carpal alignment
- Cartilage status
Age-Based Approach
Young Patients (<20 years)
- Good revascularization potential
- Often managed conservatively
Elderly Patients (>70 years)
- Often tolerate disease
- Surgery rarely needed
Non-Operative Treatment
Trial (3–6 months)
- Immobilization
- Activity modification
- NSAIDs
- Splinting
Joint Leveling Procedures
Radial Shortening Osteotomy
- Indication:
- Negative ulnar variance
- Effect:
- Reduces load on lunate
Capitate Shortening Osteotomy
- Indication:
- Neutral or positive ulnar variance
- Effect:
- Load redistribution
Radial Closing Wedge Osteotomy
- Indication:
- Increased radial inclination
- Effect:
- Alters wrist load mechanics
Reconstructive Procedures
Indication
- Lunate salvageable
Options
- Cancellous bone graft
- Vascularized bone graft
Common Graft
- 1,2-ICSRA graft
Multimodal Approach
Combination
- Joint leveling
- Vascularized graft
- Temporary K-wire stabilization
Goal
- Protect and revascularize lunate
Internal Fixation
Indications
- Young patients
- Two-part fractures
- Preserved vascularity
Limitation
- Technically difficult
Salvage Procedures
Proximal Row Carpectomy (PRC)
- Removes:
- Scaphoid
- Lunate
- Triquetrum
Advantages
- Preserves partial wrist motion
- Technically simple
Scaphocapitate Fusion
- Offloads lunate
- Preferred in young active patients
Total Wrist Fusion
- For severe arthritis
- Provides pain relief but no motion
Dynamic Factors in Disease Progression
- Carpal instability
- Dynamic impingement
- Lunate fragmentation
- Carpal translocation
- Ulnar styloid impingement
Leads to progressive collapse
Key Pathophysiological Components
- Osseous structure
- Articular cartilage
- Vascular supply
- Venous drainage
- Trabecular microstructure
- Wrist biomechanics
Key Takeaways
- Kienböck disease is multifactorial osteonecrosis
- Negative ulnar variance increases risk
- Venous congestion plays a central role
- Early stages — load reduction + revascularization
- Advanced stages — reconstructive or salvage procedures


Leave a Reply