Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
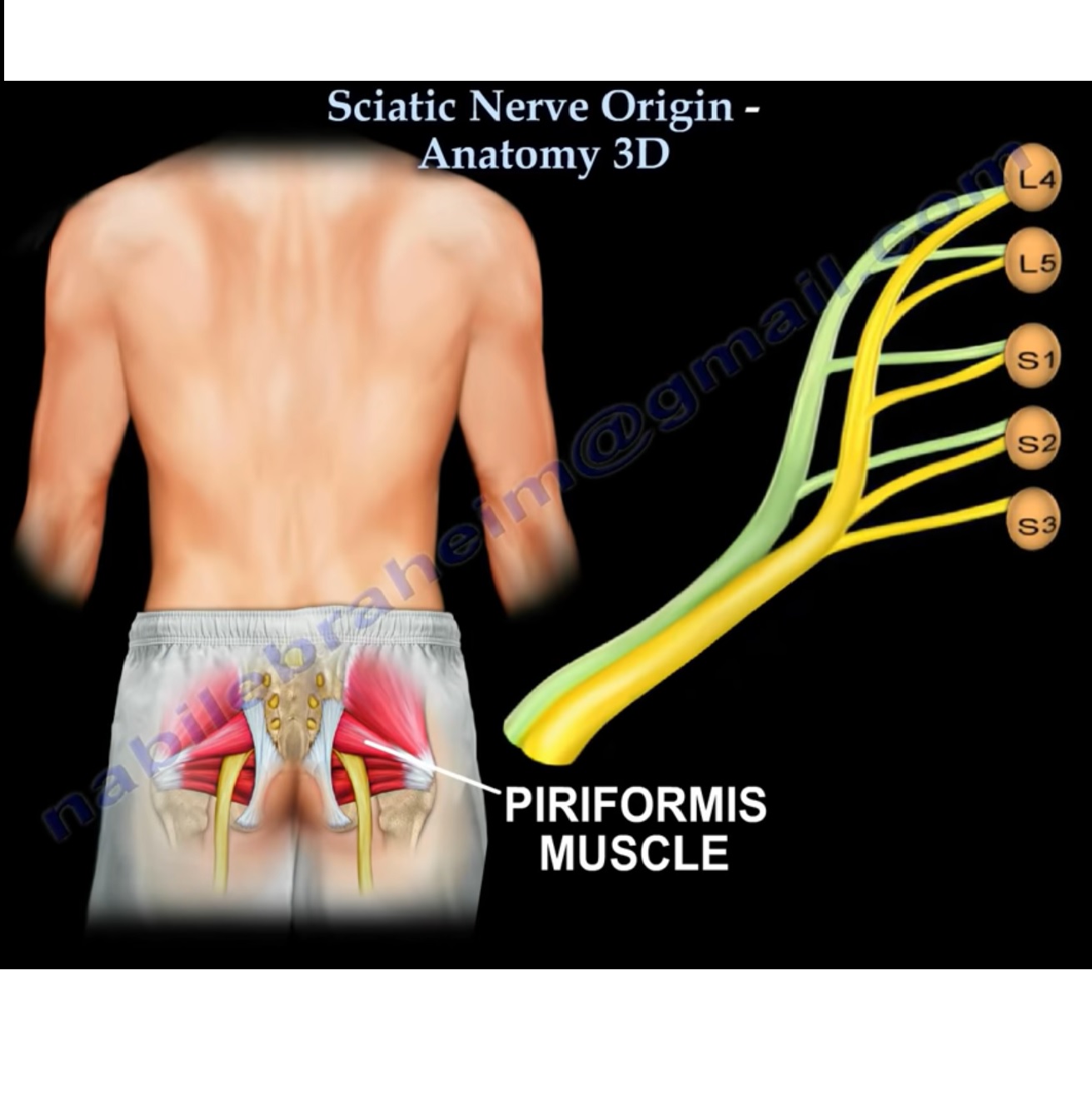
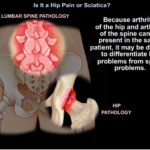
Hip Pain vs Sciatica (Spine) – Clinical Differentiation
Introduction
Hip and lumbar spine disorders commonly coexist and frequently produce overlapping symptoms.
The primary clinical goal is to identify the main pain generator:
- Hip pathology
- Spine pathology
- Or both simultaneously
Failure to recognize dual pathology may lead to incorrect treatment and persistent symptoms.
Core Clinical Differences
| Feature | Hip Pathology | Spine Pathology (Sciatica / Stenosis) |
|---|---|---|
| Pain location | Groin | Buttock or low back |
| Pain radiation | Thigh ± below knee | Dermatomal leg pain |
| Gait | Antalgic limp | Forward-flexed posture |
| Posture | Usually normal | Leaning forward |
| Hip range of motion | Reduced | Usually preserved |
| Neurological signs | Usually absent | May be present |
| Key clue | Groin pain | Radiculopathy |
Clinical Features Suggesting Hip Pathology
Groin Pain
Groin pain is the single most important clue suggesting hip pathology.
It is approximately seven times more likely to originate from the hip than the spine.
Limping Gait
Patients commonly develop:
- Antalgic gait
- Reduced weight bearing
Reduced Hip Range of Motion
Especially:
- Internal rotation
- Flexion
Pain reproduced by hip movement strongly suggests hip disease.
Functional Difficulties
Patients may complain of difficulty:
- Putting on shoes
- Sitting cross-legged
- Climbing stairs
Trochanteric Pain
Pain over the greater trochanter suggests:
- Trochanteric bursitis
- Gluteal tendinopathy
Clinical Features Suggesting Spine Pathology
Pain Location
Commonly involves:
- Buttock
- Low back
Radicular Symptoms
Features include:
- Dermatomal pain
- Paresthesia
- Numbness
- Weakness
Neurological Deficits
May include:
- Sensory loss
- Reflex changes
- Motor weakness
Postural Relief
Pain relieved by:
- Sitting
- Forward bending
strongly suggests lumbar spinal stenosis.
Neurogenic Claudication
Cause
Usually due to:
- Lumbar spinal stenosis
Clinical Features
Symptoms include:
- Leg heaviness
- Cramping
- Pain during walking
Symptoms worsen with:
- Standing
- Walking
Symptoms improve with:
- Sitting
- Leaning forward
Shopping Cart Sign
Patients often report symptom relief while leaning on a shopping cart.
This is a classic sign of lumbar spinal stenosis.
Classic Features of Hip Arthritis
Typical findings include:
- Groin pain
- Limp
- Reduced hip range of motion
- Antalgic gait
Loss of internal rotation is often an early sign.
Important Clinical Pitfalls
Patient Description of “Hip Pain”
Patients may describe:
- Buttock pain
- Sacroiliac pain
- Trochanteric pain
as “hip pain.”
Precise localization is essential.
Imaging Pitfall
Degenerative changes on:
- X-ray
- MRI
may not represent the actual pain source.
Always correlate imaging with clinical findings.
Diagnostic Strategy
Step 1: Detailed History and Examination
Ask the patient to point to the exact pain location.
Different locations suggest different pathology:
| Pain Location | Likely Source |
|---|---|
| Groin | Hip joint |
| Lateral hip | Trochanteric bursitis |
| Buttock | Spine or SI joint |
Step 2: Evaluate Both Regions
Always assess:
- Hip in spine patients
- Spine in hip patients
Dual pathology is common.
Step 3: Diagnostic Injection
When diagnosis remains uncertain, intra-articular hip injection is highly useful.
Interpretation
Significant Pain Relief
Suggests:
- Hip joint is the primary pain source
No Pain Relief
Suggests:
- Spine pathology is more likely
Diagnostic injection is often considered the clinical tie-breaker test.
Trochanteric Bursitis
Clinical Features
- Lateral hip pain
- Tenderness over greater trochanter
- Pain while lying on affected side
More common in women.
Key Clinical Pearls
- Groin pain strongly suggests hip pathology.
- Buttock pain more commonly suggests spine or SI joint pathology.
- Limping favors hip disease.
- Radiculopathy favors spinal pathology.
- Forward-flexed posture suggests lumbar spinal stenosis.
- Reduced hip internal rotation is an important sign of hip arthritis.
- Imaging findings alone should never determine treatment.
- Always consider coexistence of hip and spine pathology


Leave a Reply