Courtesy: Dr Prabhudevprasad Purudappa, MD
Instability in Total Hip Replacement (THR)
Overview
Instability remains one of the most common and challenging complications following total hip replacement. Complication rates after primary total hip arthroplasty (THA) range from 2% to 10%, with the most frequent causes being:
-
Aseptic loosening – 36.5%
-
Dislocation – 17.7%
-
Infection – 15.3%
Definition of Instability
Dislocation
-
Complete loss of contact between the femoral head and acetabular component
-
May result from:
-
A significant traumatic force in an otherwise stable joint
-
Progressive culmination of unstable conditions in arthroplasty
-
-
Requires intervention for reduction
Subluxation
-
Sensation of incomplete or transient displacement
-
Occurs during routine daily activities
-
Does not require unusual or extreme forces
-
Self-reducing with spontaneous restoration of normal joint congruity
Incidence
-
Annual incidence of dislocation after primary THA ranges from 0.2% to 10%
-
Majority occur within the first 3 months
-
Cumulative risk:
-
First month: ~1%
-
First year: ~2%
-
Increases by ~1% every 5 years
-
Approximately 7% at 25 years
-
Risk Factors for Instability
Patient-Related Risk Factors
-
Female sex (controversial)
-
Advanced age (>80 years)
-
Obesity
-
Femoral neck fractures
-
Neuromuscular or cognitive disorders
-
Generalized ligamentous laxity or connective tissue disorders
-
Alcohol abuse
-
Prior hip surgery
-
Rapidly progressive or inflammatory arthropathies
-
Osteonecrosis of the femoral head
-
Reduced spinopelvic mobility
Risk Factor – Intervention Strategies
| Risk Factor | Preventive Strategy |
|---|---|
| Tobacco / alcohol abuse | Preoperative cessation counseling |
| Advanced age | Dual mobility liner |
| Obesity | Weight reduction programs |
| Neuromuscular disorders / CTDs | Dual mobility liner |
| Reduced spinopelvic mobility | Larger femoral heads (>32 mm) |
| Optimized component anteversion and inclination | |
| Robotic or navigation-assisted implantation |
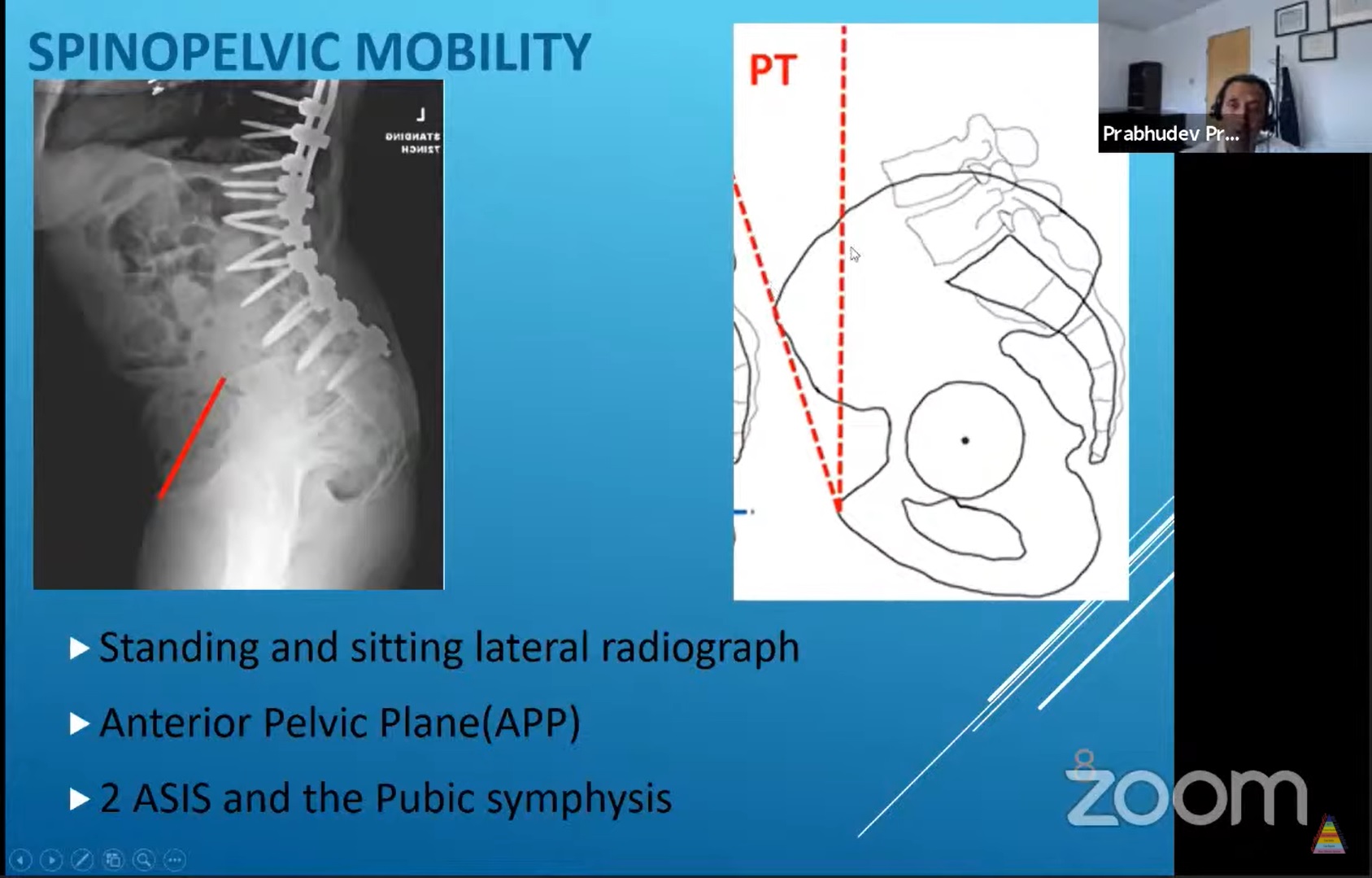
Spinopelvic Mobility
Key Parameters
Pelvic Tilt
-
Angle between the anterior pelvic plane (ASIS and pubic symphysis) and the coronal plane
-
Measured on lateral standing and sitting radiographs
Sacral Slope
-
Angle between the superior endplate of the sacrum and the horizontal plane
Normal Values
-
Change in posterior pelvic tilt and sacral slope: 20–35° from standing to sitting
-
For each degree increase in posterior pelvic tilt (or decrease in sacral slope), acetabular anteversion increases by 0.7–0.8°
Stiff Spine
-
Reduced, absent, or paradoxical pelvic tilt
-
<10° change in sacral slope between standing and sitting
-
Significantly increases risk of instability
Procedure-Related Risk Factors
-
Surgical approach
-
Component positioning
-
Soft tissue tension
-
Quality of soft tissue repair
-
Surgeon experience
Implant-Related Risk Factors
-
Femoral head size
-
Prosthetic impingement
Surgical Approach
-
Meta-analysis of 25 studies (7,000 patients) comparing direct anterior approach (DAA) and posterior approach (PA) showed no significant difference in dislocation rates.
Surgeon Experience
-
Inverse relationship between surgeon volume and dislocation rate
-
For every 10 additional THAs performed annually, postoperative dislocation rate decreases by ~50%
-
Highest dislocation rates seen in surgeons performing <30 THAs per year
Soft Tissue Repair
-
Meticulous posterior soft tissue repair in posterior approach reduces dislocation risk by up to 10-fold
-
Well-repaired posterior capsule: <1% dislocation rate
Component Positioning
Acetabular Component
-
Correct depth (mediolateral position)
-
Appropriate height (superoinferior position)
-
Proper inclination and anteversion
Femoral Component
-
Correct varus/valgus alignment
-
Appropriate version
Optimal Cup Positioning
-
Dislocation rate:
-
1.5% when cup lies within the safe zone
-
6.1% when outside the safe zone
-
-
Safe zone:
-
Anteversion: 5–25°
-
Inclination: 30–50°
-
-
Combined anteversion:
-
Ideal: 40–60°
-
Risk increases 6.9-fold when outside this range
-
Soft Tissue Tension
The goal of THR is restoration of:
-
Center of rotation
-
Offset
-
Limb length
-
Abductor integrity
This restores physiological soft tissue tension and stability.
Templating
-
Conventional two-dimensional templating is imprecise
-
Purpose extends beyond implant sizing to:
-
Optimizing cup position
-
Restoring center of rotation
-
Correcting height, depth, and angular alignment
-
Patient Positioning
-
Most THAs performed in lateral decubitus position
-
Pelvic tilt can vary from 25° posterior to 20° anterior
-
Stabilization of ASIS, pubic symphysis, and sacrum is essential
Navigation and Robotics
-
Increase accuracy of component placement
-
Higher percentage of cups within safe zone
-
Reduced dislocation rates
-
Limitations: cost and increased operative time
Transverse Acetabular Ligament (TAL)
-
Reliable intraoperative landmark for acetabular version
-
Target combined anteversion: 30–45°
-
<30° -posterior instability
-
45° – anterior instability
-
Evaluation of an Unstable THA
History
-
Mechanism of dislocation
-
Infective symptoms
-
Surgical approach used
-
Intraoperative or postoperative complications
-
Prior imaging and documentation
Physical Examination
-
Spinal deformities
-
Gait abnormalities
-
Pelvic obliquity (fixed or mobile)
-
Soft tissue contractures
-
Abductor strength
-
Distal neurological status
Infection Work-up
-
ESR, CRP
-
Joint aspiration and cultures when in doubt
Radiographic Evaluation
Assess:
-
Cup inclination
-
Cup offset (center of rotation to teardrop)
-
Stem offset
-
Height of hip center
-
Stem alignment and subsidence
-
Acetabular and femoral anteversion
CT scan is the gold standard when plain radiographs are inconclusive.
Diagnosis
-
Early vs late instability
-
Traumatic vs atraumatic
-
Anterior vs posterior
-
Component-related vs soft tissue-related
Management
Non-Surgical Treatment
-
Closed reduction under anesthesia
-
Post-reduction imaging to confirm concentric reduction
-
Bracing (hip spica, knee immobilizer) for 6 weeks
-
Success:
-
No recurrence: ~67%
-
Recurrence: ~33%
-
Irreducible: 3–6%
-
Indications for Surgery
-
>2 dislocations
-
Failed conservative treatment
-
Irreducible dislocation
-
Malpositioned components
-
Inadequate soft tissue tension
-
Failure to achieve concentric reduction
Surgical Options
-
Revision of components
-
Modular exchange (head and liner)
-
Removal of impingement
-
Larger femoral heads
-
Dual mobility liners
-
Constrained liners
-
Soft tissue reinforcement
-
Girdlestone resection arthroplasty
Take-Home Messages
-
Instability after THR is multifactorial
-
Proper preoperative planning, component positioning, and soft tissue management are critical
-
Closed reduction and bracing are effective in most first-time dislocations
-
Successful revision surgery depends on accurate identification and correction of the underlying cause

Leave a Reply