Courtesy: Nijil Vasukutty, FRCS Orth, United Lincolnshire Hospitals, UK
Infections of the Foot and Ankle
Overview
- Foot and ankle infections range from superficial to life-threatening conditions
- Early diagnosis and prompt treatment are essential to prevent:
- Limb loss
- Systemic complications
Systematic Approach to Infection
Evaluate Based on Three Key Factors
1. Location
- Skin
- Soft tissue
- Bone
- Joint
2. Causative Organism
- Bacterial (most common)
- Fungal
- Mycobacterial
3. Host Factors
- Age
- Comorbidities (e.g., diabetes)
- Immune status
- Overall health
Anatomical Classification of Infections
Superficial Infections
- Nail infections (onychomycosis)
- Epidermal infections (tinea pedis / athlete’s foot)
- Dermal infections (cellulitis)
Deep Infections
- Necrotizing fasciitis
- Osteomyelitis
- Septic arthritis
Common Superficial Infections
1. Onychomycosis
Definition
- Fungal infection of the nail
Diagnosis
- Nail clippings or scrapings
Management
- Topical antifungal therapy
- Systemic antifungal therapy
- Surgery (selected cases)
2. Tinea Pedis (Athlete’s Foot)
Clinical Features
- Itching
- Scaling
- Commonly between toes
Variants
- Hyperkeratotic type
- Vesicular type
3. Cellulitis
Clinical Features
- Redness
- Warmth
- Tenderness
- Swelling
Common Organisms
- Streptococci
- Staphylococci
Spread
- May involve lymphatic system
Serious Soft Tissue Infection
Necrotizing Fasciitis
Characteristics
- Rapidly progressive
- Life-threatening
Key Clinical Features
- Severe pain disproportionate to findings
- Blisters
- Skin necrosis
- Crepitus
- Systemic toxicity
Risk Factors
- Diabetes
Management
- Early recognition
- Urgent surgical debridement
- Broad-spectrum antibiotics
- Hemodynamic stabilization
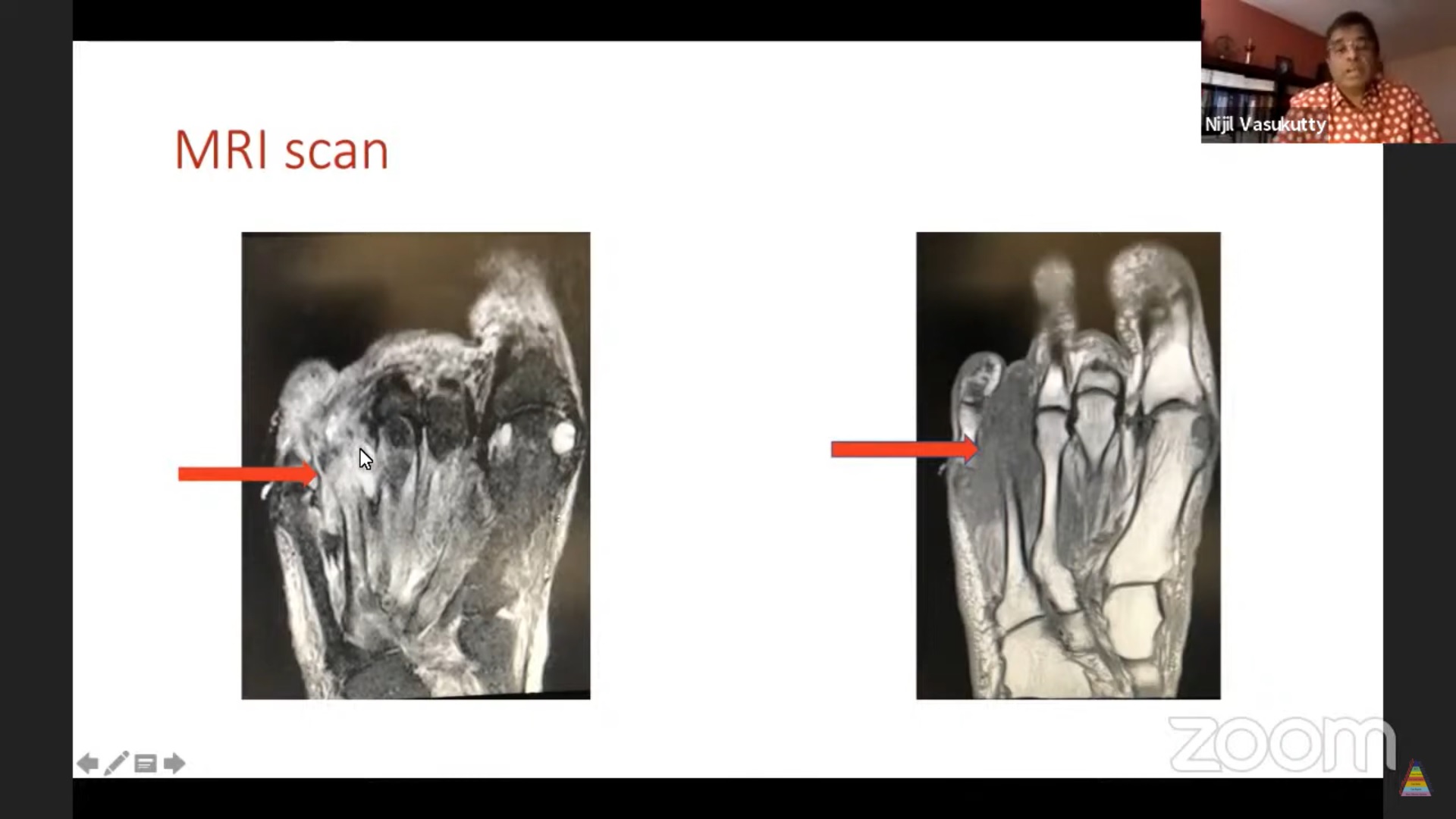
Bone Infection (Osteomyelitis)
Routes of Infection
- Hematogenous (common in children)
- Direct inoculation (trauma/surgery)
- Contiguous spread (e.g., diabetic ulcers)
Disease Progression
- Begins in bone marrow
- Extends to cortex and periosteum
- Leads to:
- Abscess
- Sequestrum
- Involucrum
- Sinus formation
Diagnosis
- Early:
- MRI
- Late:
- X-ray
Management
- Culture-directed antibiotics
- Surgical debridement (if required)
Diabetic Foot Infections
Epidemiology
- Increasing global burden
- High morbidity and mortality
Pathophysiology
- Combination of:
- Sensory neuropathy — loss of protective sensation
- Motor neuropathy — deformity
- Autonomic neuropathy — dry skin
Classification
Based On
- Ulcer depth
- Presence of infection
- Presence of ischemia
Principles of Management
Multidisciplinary Approach
- Physicians
- Surgeons
- Microbiologists
- Radiologists
- Wound care specialists
Core Treatment Components
1. Wound Care
- Debridement of necrotic tissue
2. Antibiotics
- Culture-guided therapy
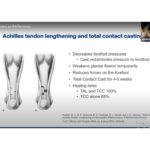
3. Offloading
- Prevent weight-bearing
4. Vascular Assessment
- Ensure adequate blood supply
5. Metabolic Control
- Optimize blood glucose
6. Patient Education
- Prevent recurrence
Surgical Management
Principles
- Early and aggressive debridement
- Remove all non-viable tissue
- Obtain samples for culture
Reconstruction
- Grafts or flaps after infection control
Advanced Therapies
Local Antibiotic Delivery
- High local concentration
- Reduced systemic side effects
Negative Pressure Wound Therapy (VAC)
- Promotes healing
- Reduces edema
- Enhances granulation tissue
Special Clinical Situations
Foot Attack
- Acute severe infection
- Requires emergency debridement
Heel Ulcers
- Difficult due to poor vascularity
- May require bone resection
Less Common Infections
- Tuberculosis of bone and joints
- Mycetoma (Madura foot)
When to Suspect
- Non-healing wounds
- Atypical presentation
Antibiotic Stewardship
- Avoid overuse
- Use culture-guided therapy
- Be aware of:
- Biofilm-related resistance
Key Takeaways
- Always follow a structured approach:
- Location
- Organism
- Host factors
- Early diagnosis is critical
- Multidisciplinary care improves outcomes
- Surgical debridement is often essential
- Offloading and patient education are key to prevention


Leave a Reply