HUNTINGTONS PROCEDURE
- Also known as ipsilateral vascularized fibula transfer used to reconstruct large tibial defect ,particularly in children.
- Usually involves using fibula bone from the same leg to replace a section of tibia that is missing or damaged
- First suggested by Kahn in 1884 for pseudoarthrosis of tibia
• First successfully done by Huntington in 1903 to fill a 12.7cm tibial defect in a 7 year old boy
• Popularized the technique as a two stage procedure in 1944 for the treatment of tibial defect in children.
• Adopted in Orthopaedic oncology and trauma
INDICATIONS
Segmental long bone defect due to :-
1. Tumor resection
2. High energy trauma
3. Infected non union
4. Congenital pseudoarthrosis
5. Failed reconstructions
PRE REQUISITES
• Tibial defect of size >4cm with intact fibula
• No distal neurovascular deficits
• Adequate tibial stump at both proximal and distal level for fixation of fibula
• Complete elimination of the infection from tibia.
CONTRAINDICATIONS
• Poor vascularity of limb
• Previous fibular harvest or damage
• Active infection at recepient or donor site
• Poor general conditions
PRINCIPLES
• Based on sound principles of good fixation, control of infection and an environment favorable to bone healing.
• Usually recommended for paediatric patients as the fibular graft in adult patients is considered to be inadequate in terms of size and strength.
• Large graft of ipsilateral fibula which is first raised onto the pedicle of the peroneal artery and then aligned and fixed to the tibia in the posterior aspect provides a sound mechanical and biological basis for the union.
• Subperiosteal dissection is performed at the osteotomy site and the remaining muscular attachments to the fibula are left intact.
• Fibula is not devascularised completely and there is always a free blood supply to the other end of the transported fibula . This also supports fibular hypertrophy and union at the synostotic site, which later substitutes for a defective tibia.
• The reduction in lower leg volume due to the anteromedial shift of the fibula makes skin closure easier, even in patients with scarred tissue
• Now it is performed as a single stage procedure. But, for a single- stage procedure extensive soft tissue release can jeopardise blood supply.In the two-stage procedure, even if the extensive soft tissue release is performed only at one synostosis site, the fibula blood supply from other end will remain intact, facilitating healing at the synostotic site.
PRE OPERATIVE EVALUATION
• Routine blood test:- CBC,ESR,CRP,blood c/s to rule out infection.
• XRAYS,CT and MRI for defect evaluation
• CT angiography and Doppler study for vascular mapping
• Councelling and informed consent
TECHNIQUE
• Done in 2 stages
• First stage:-Synostosis between the proximal tibial fragment and the fibula.
• Two incisions are made – a lateral incision to expose the proximal fibula and anterior incision to expose the distal lateral proximal tibia
• A trough is prepared to recieve the proximal end of the fibula by slanting the small osteotome upwards and inwards. Fibula is osteotomized at a slightly higher level than proximal edge of the tibial trough.
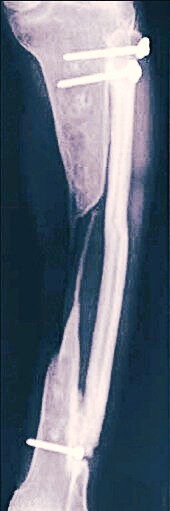
• The proximal end of the fibular graft is fitted into the trough and secured with one or two screws or k wires
• Second Stage:- Conducted as a similar procedure by fixing the distal end of the fibular graft into the prepared slot and reinforcement with screws or k wires. Second stage is done at 2-4 months after the first stage.
• Now a days it is performed as a single stage procedure also.
POST OPERATIVE MANAGEMENT
• Limb elevation
• Neurovascular checks
• Monitor perfusion for 72 hours
• Antibioics,DVT prophylaxis
• Pain and infection control
• Immobilized by external fixator for 3 months followed by above knee cast for 6 weeks and then PTB cast for another 6 weeks
• Healing of the transferred fibula was evaluated radiographically
• Immobilization continues until radiographic healing is evident(usually by 14 weeks)
VARIANTS AND MODIFICATIONS
• Double-barrel fibula(reconstructive procedure of mandible)
• Hybrid fixation (plate + external fixator)
• With bone transport (Ilizarov)
REHABILITATION PROTOCOL
• Week 0-6 -Immobilization,no weight
• Week 6-12 -Partial weight bearing if healing
• After 6 months -Gradual full weight bearing
ADVANTAGES
• Biological-Uses vascularized bone giving better healing capacity
• Cost-effective
• Minimal implants needed-Simple fixation using screws and bone graft
• Bone remodels with weight bearing and hypertrophies
LIMITATIONS
• Long treatment -12 -18 months to reach full weight bearing
• Patient selection-Not ideal for compromised circulation,elderley or with poor soft tissue coverage
COMPLICATIONS
• Breakage of screws and k wires
• Proximal migration of fibula leading to knee
• subluxation
• Stress fractures in transfered fibula
• Non union at proximal or distal sites
• Recurrent infections
• Mal-alignment in proximal and distal tibia
ALTERNATIVE PROCEDURES
• Non-vascularized grafts
• Endoprosthesis
• Bone transport
• Allografts


Leave a Reply