Courtesy: Baljinder Dhinsa, FRCS Tr and Orth, Kent, UK
Definition
Hallux rigidus is a painful degenerative condition of the first metatarsophalangeal (MTP) joint.
Key Features
- Restricted range of motion (especially dorsiflexion)
- Periarticular osteophyte formation
- Progressive degenerative arthritis
Terminology
- Hallux limitus
- Dorsal bunion
- Metatarsus primus elevatus
Hallux rigidus is preferred as it reflects global joint stiffness
Epidemiology
General Trends
- Most common arthritic condition of the foot
- Often bilateral
Age Groups
- Adolescents – often osteochondral origin
- Adults – degenerative arthritis
Genetic Influence
- Up to 50% familial history in adolescents
- ~80% report family history of great toe disorders
Etiology
Primary Cause
- Often idiopathic
Trauma-Related Causes
Acute Trauma
- Hyperextension injury
- Impaction of proximal phalanx
Repetitive Microtrauma
- Progressive cartilage damage
Proposed Anatomical Factors (Inconclusive)
- Flattened metatarsal head
- Abnormal metatarsal length
- Pes planus
- Hindfoot pronation
- Tight intrinsic muscles
Clinical Features
History
- Pain at first MTP joint
- Swelling (early)
- Progressive stiffness
- Difficulty during:
- Walking
- Push-off phase
Footwear Difficulty
- Due to dorsal osteophytes
- Shoe irritation
Neurological Symptoms
- Dorsal digital nerve irritation
- Tingling or hyperesthesia
Associated Conditions
- Transfer metatarsalgia
- Hallux valgus deformity
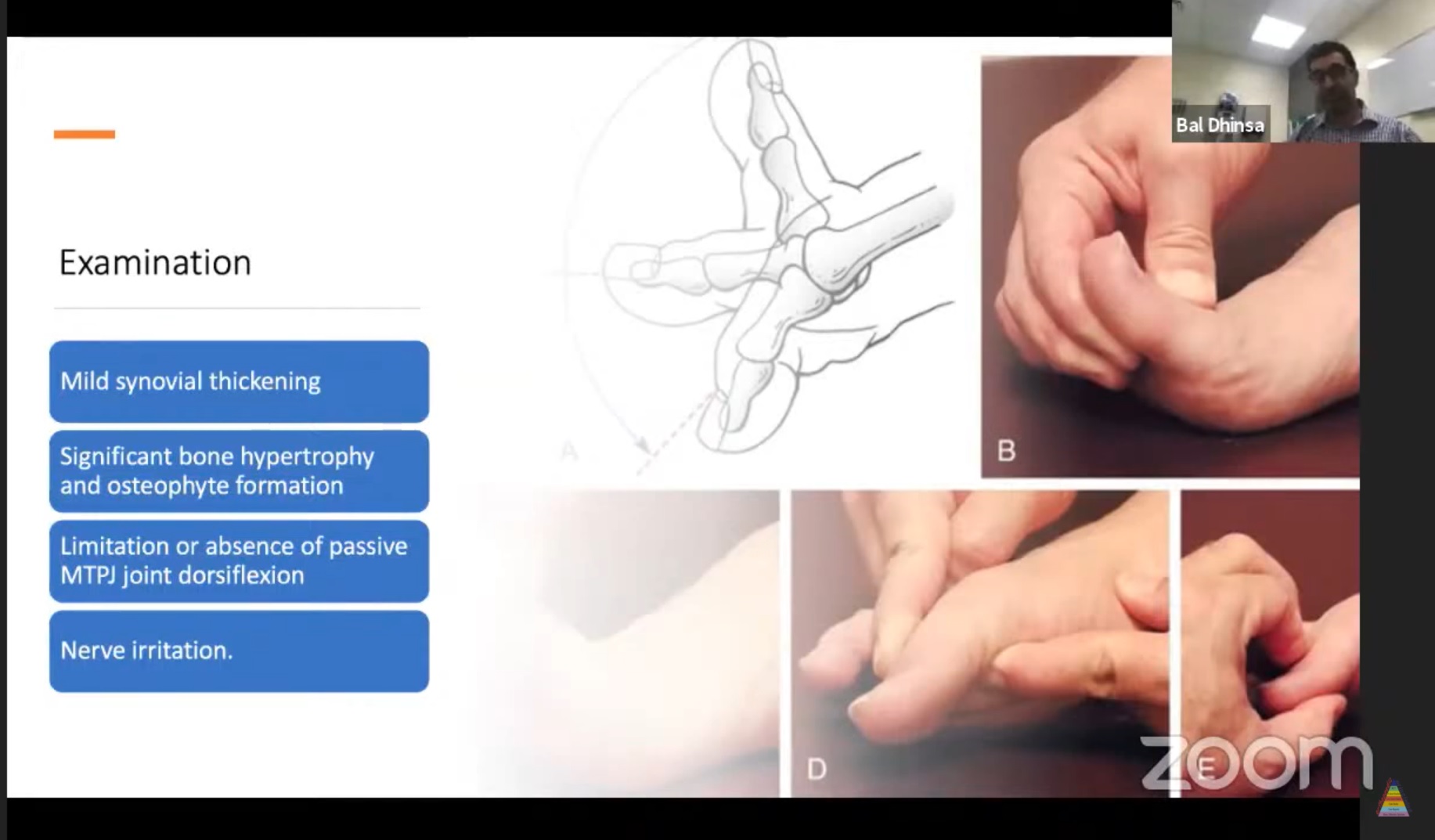
Clinical Examination
General Assessment
- Gait analysis
- Footwear inspection
- Orthotic use
- Wear pattern
Alignment Assessment
- Hindfoot
- Midfoot
- Forefoot
Local Examination
Early Stage
- Synovial thickening
- Mild swelling
Advanced Stage
- Dorsal osteophytes
- Bony prominence
- Reduced motion
Movement Findings
- Marked loss of dorsiflexion
- Pain:
- Dorsiflexion — impingement
- Plantarflexion — capsular stretch
Neurological Signs
- Dorsal nerve irritation
- Tinel-like sign
Imaging
Plain Radiographs (Essential)
Weight-Bearing Views
- AP
- Lateral
- Medial oblique
Radiographic Findings
Lateral View
- Dorsal osteophytes
- “Candle wax” spur
Oblique View
- Better visualization of joint space
AP View
Early Stage
- Non-uniform joint space narrowing
- Early osteophytes
Advanced Stage
- Subchondral sclerosis
- Cysts
- Osteophytes
- Enlarged proximal phalanx base
MRI
- Early disease
- Osteochondral lesions
- Cartilage assessment
CT / Ultrasound / Bone Scan
- Limited or no routine role
Pathophysiology
Early Changes
- Chondrocyte dysfunction
- Inflammatory mediators:
- IL-1
- TNF
Cartilage Effects
- Proteoglycans
- Type II collagen
- Water content
Cartilage becomes:
- Soft
- Friable
- Fissured
Progression
- Cartilage loss
- Subchondral bone exposure
- Osteophyte formation
- Synovitis
Classification (Coughlin & Shurnas)
Grading (0–4)
Based on:
- Range of motion
- Radiological findings
- Clinical symptoms
Key Concept
- Early disease pain dominant
- Late disease stiffness dominant
Non-Operative Management
Trial Duration
- 6–12 months
Footwear Modifications
- Wide toe box
- Stiff sole
- Rocker-bottom shoes
Orthoses
- Carbon fiber plate
- Morton’s extension
Reduce MTP motion
Medications
- NSAIDs
- Topical agents
Injections
Corticosteroids
- Temporary relief (~6 months)
Hyaluronic Acid
- Limited evidence
Surgical Management
1. Cheilectomy
Indications
- Grade I–II disease
Procedure
- Remove:
- Dorsal metatarsal head (1/3)
- Osteophytes
Outcomes
- Pain relief in 90–97%
- Limited ROM improvement (~40° dorsiflexion)
Advantages
- Day-case procedure
- Early weight-bearing
Limitations
- Possible progression to arthritis
2. Moberg Osteotomy
Procedure
- Dorsiflexion osteotomy of proximal phalanx
Indications
- Early disease (Grade I–II)
Outcome
- High satisfaction (~99%)
Limitation
- Difficult conversion to arthrodesis
3. Keller Resection Arthroplasty
Procedure
- Resection of proximal phalanx base
Complications
- Weak push-off
- Transfer metatarsalgia
- Cock-up deformity
Now less commonly used
4. Interposition Arthroplasty
Technique
- Soft tissue interposition
Limitations
- Persistent weakness
- Declining popularity
5. Implant Arthroplasty
Types
- Silastic
- Metal
- Ceramic
- Synthetic cartilage
Problems
- Osteolysis
- Subsidence
- High revision rates
Cartiva Implant
- Hydrogel implant
Advantages
- Preserves bone
- Easier revision
Outcome
- Good short-term results
- ~9% revision at 2 years
6. Arthrodesis (Gold Standard)
Indications
- Grade III–IV disease
- Severe arthritis
- Failed prior surgery
Optimal Position
- 10–15° dorsiflexion (floor)
- 20–25° relative to metatarsal
- 5–15° valgus
Fixation Options
- Cross screws
- Plate + screw (strongest)
- Staples
Outcomes
-
90–96% satisfaction
- High union rates
Return to Activity
- Hiking – 92%
- Golf – 80%
- Tennis/jogging ~75%
Practical Treatment Algorithm
Stage-Based Approach
- Stage I – Cheilectomy
- Stage II – Cheilectomy ± Moberg
- Stage III–IV – Arthrodesis
Key Take-Home Points
- Hallux rigidus = degenerative arthritis of 1st MTP joint
- Early – pain; Late – stiffness
- Radiographs are essential for diagnosis
- Conservative treatment is first-line
- Arthrodesis is the most reliable treatment for advanced disease

Leave a Reply