Courtesy: Baljinder Dhinsa, FRCS Tr and Orth, Kent, UK
Definition
- Hallux rigidus is a painful degenerative condition of the first metatarsophalangeal (MTP) joint.
- Characterized by:
- Restricted range of motion, especially dorsiflexion
- Periarticular osteophyte formation
- Progressive degenerative arthritis of the first MTP joint
- First described in 1887.
- Other related terms:
- Hallux limitus
- Dorsal bunion
- Metatarsus primus elevatus
- Hallux rigidus is preferred because it reflects global stiffness rather than isolated limitation.
Epidemiology
- Most common arthritic condition of the foot.
- May occur in:
- Adolescents (often associated with osteochondral defects)
- Adults (usually degenerative arthritis).
- Studies report familial predisposition:
- Up to 50% family history in adolescents.
- Approximately 80% of patients may report family history of great toe disorders.
- Bilateral involvement is common.
Etiology
The exact cause remains unclear.
Trauma
- Acute trauma
- Hyperextension injury of the first MTP joint.
- Impaction of the proximal phalanx against the metatarsal head.
- Repetitive microtrauma
- Leads to progressive cartilage damage.
Proposed Anatomical Associations (not proven)
- Flattened or squared metatarsal head
- Long or short first metatarsal
- Tight intrinsic muscles
- Pes planus
- Hindfoot pronation
- Congruent first MTP joint
Evidence for these associations remains inconclusive.
Clinical Features
History
Patients commonly complain of:
- Pain in the first MTP joint
- Swelling in early stages
- Progressive stiffness
- Reduced dorsiflexion
- Pain during:
- Walking
- Push-off phase of gait
- Difficulty wearing shoes due to:
- Dorsal bony prominence
- Shoe friction over osteophytes
Neurological symptoms
- Compression of dorsal cutaneous nerve
- May cause:
- Tingling
- Hyperesthesia
- Local irritation
Associated symptoms
- Transfer metatarsalgia
- Development of hallux valgus deformity
- Secondary soft-tissue irritation
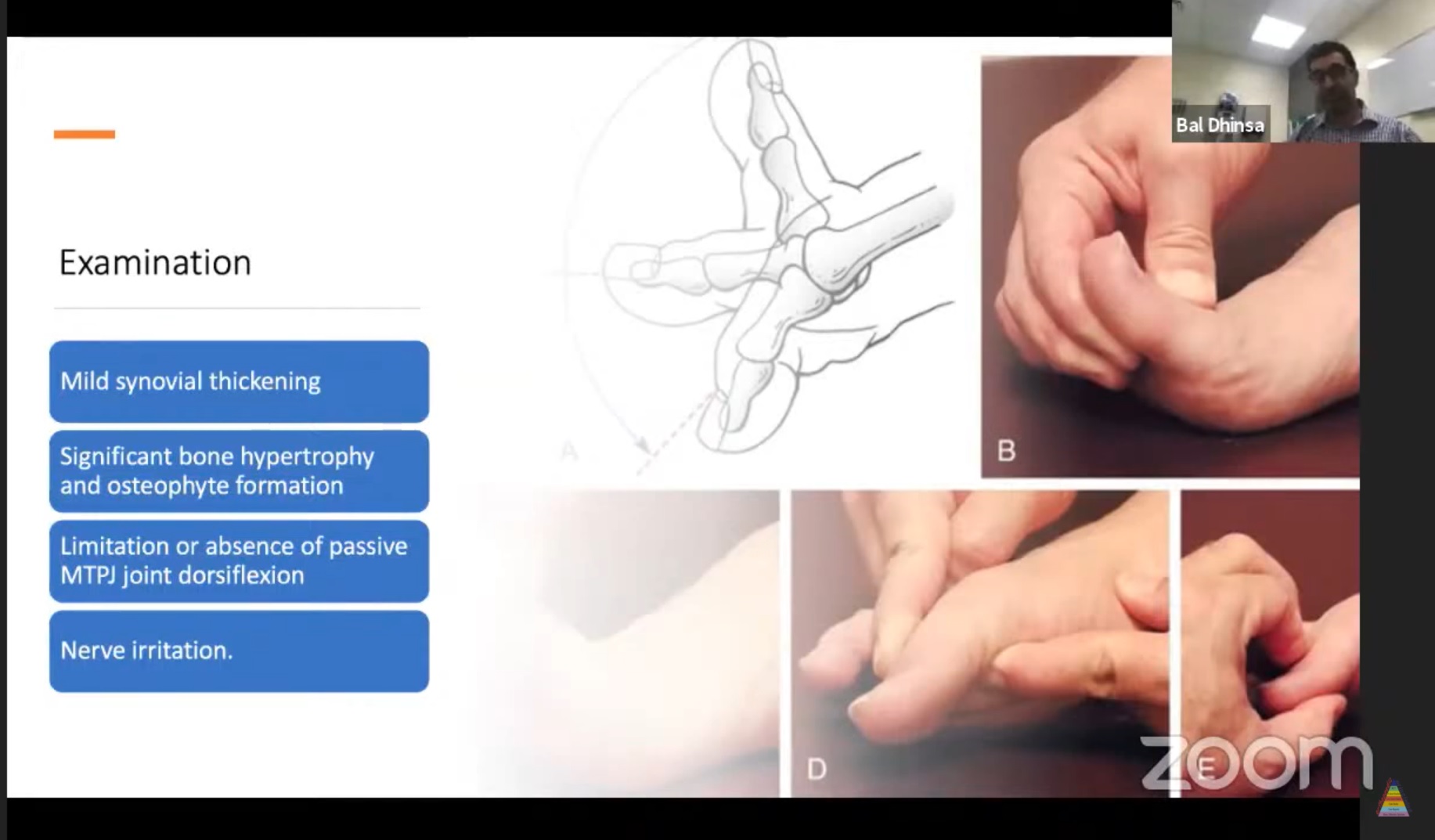
Clinical Examination
General Examination
Follow standard FRCS foot examination:
- Assess gait
- Inspect footwear
- Look for orthoses
- Examine wear patterns
Foot Alignment
Assess:
- Hindfoot
- Midfoot
- Forefoot alignment
Local Examination
Early Disease
- Synovial thickening
- Mild swelling
Progressive Disease
- Dorsal osteophytes
- Bony prominence (often dorsolateral)
- Reduced range of motion
Movement
- Marked restriction of dorsiflexion
- Pain with:
- Dorsiflexion (bony impingement)
- Plantarflexion (capsular stretching)
Neurological Signs
- Irritation of dorsal digital nerve
- Possible Tinel-like sign
Vascular and Neurological Assessment
- Palpate peripheral pulses
- Assess sensory function
Imaging
Plain Radiographs (Essential)
Weight-bearing:
- AP view
- Lateral view
- Medial oblique view
Lateral View
- Dorsal osteophytes
- Spur formation resembling “candle wax” projection
Oblique View
- Useful when AP view is obscured by osteophytes
- Helps assess true joint space
AP View Findings
Early stage:
- Non-uniform joint space narrowing
- Early osteophyte formation
Advanced stage:
- Subchondral sclerosis
- Subchondral cysts
- Osteophytes
- Enlargement of proximal phalanx base
MRI
Indications:
- Early disease
- Suspected osteochondral defect
- Cartilage evaluation
CT Scan
- Limited role in routine assessment.
Ultrasound
- Rarely required.
Bone Scan
- No routine role.
Pathophysiology of Degenerative Changes
- Disease begins with cartilage and chondrocyte dysfunction.
- Early stages:
- Chondrocyte proliferation
- Release of inflammatory mediators:
- Interleukin-1
- Tumor necrosis factor
- These inhibit:
- Proteoglycan synthesis
- Type II collagen production
Cartilage Changes
- Increased water content
- Decreased proteoglycans
- Cartilage becomes:
- Soft
- Friable
- Fissured
Progressive Degeneration
- Cartilage fragmentation
- Exposure of subchondral bone
- Development of:
- Subchondral cysts
- Osteophytes
- Synovial inflammation
Classification (Coughlin and Shurnas)
Grades 0–4 based on:
- Range of motion
- Radiographic changes
- Clinical symptoms
Key Concept
- Early disease ? pain predominant
- Advanced disease ? stiffness predominant
Non-Operative Management
Trial period: 6 months to 1 year
Footwear Modification
- Wide toe-box shoes
- Stiff-soled shoes
- Rocker-bottom soles
Orthoses
- Carbon fibre plate
- Morton’s extension
Purpose:
- Reduce first MTP joint motion.
Medications
- NSAIDs
- Topical anti-inflammatory gels
Injections
- Corticosteroid injections
- Temporary relief (up to ~6 months)
- Hyaluronic acid injections
- Limited evidence of benefit.
Surgical Management
Indicated when conservative treatment fails.
Cheilectomy
Indications
- Grade I–II (early disease)
Procedure
- Removal of:
- Dorsal one-third of metatarsal head
- Osteophytes
- Dorsal proximal phalanx osteophytes
First described by DuVries (1959).
Outcomes
- Pain relief in ~90–97% of patients
- Limited improvement in ROM
- Realistic postoperative dorsiflexion:
- ~40°
Advantages
- Day-case procedure
- Early weight-bearing
- Quick recovery
Limitations
- May progress to arthritis
- Revision to arthrodesis occasionally required.
Moberg Osteotomy
Procedure
- Dorsiflexion osteotomy of proximal phalanx
- Often combined with cheilectomy.
Indications
- Grade I–II disease
Outcomes
- Satisfaction rates up to ~99%
Limitation
- Difficult conversion to arthrodesis later due to altered anatomy.
Keller Resection Arthroplasty
Procedure
- Resection of base of proximal phalanx
Complications
- Weak push-off
- Transfer metatarsalgia
- Cock-up deformity
Due to these complications, the procedure is less commonly used today.
Interposition Arthroplasty
Modification of Keller procedure.
- Limited bone resection
- Interposition using:
- Capsule
- Tendon
- Muscle
Limitations
- Persistent weakness
- Transfer metatarsalgia
- Declining popularity.
Arthroplasty (Implants)
Types
- Silastic implants
- Metal implants
- Ceramic implants
- Synthetic cartilage implants
Problems with Early Implants
- Osteolysis
- Implant subsidence
- High revision rates.
Synthetic Cartilage Implant (Cartiva)
- Synthetic hydrogel implant
- Placed in metatarsal head defect.
Advantages
- Preserves bone stock
- Easier conversion to arthrodesis.
Outcomes
- Good short-term results
- ~9% revision rate at 2 years.
Long-term data still limited.
Arthrodesis (Gold Standard)
First MTP joint fusion is considered the most reliable treatment.
Indications
- Grade III–IV disease
- Severe arthritis
- Rheumatoid arthritis
- Neuromuscular disorders
- Failed previous surgery.
Optimal Fusion Position
- 10–15° dorsiflexion relative to floor
- 20–25° dorsiflexion relative to first metatarsal
- 5–15° valgus
Toe tip should:
- Touch the floor
- Allow slight lift under the toe.
Fixation Techniques
- Crossed lag screws
- Lag screw + dorsal plate
- Locking compression plate
- Compression staples
Biomechanically strongest construct
- Lag screw + dorsal plate
Outcomes of Arthrodesis
Literature reports:
- >90–96% patient satisfaction
- High union rates
- Low revision rates.
Functional outcomes:
- 92% return to hiking
- 80% return to golf
- 75% return to tennis
- 75% return to jogging.
Practical Surgical Approach (Common Practice)
Typical surgeon preference:
- Stage I ? Cheilectomy
- Stage II ? Cheilectomy ± Moberg osteotomy
- Stage III–IV ? First MTP arthrodesis

Leave a Reply