Courtesy: Orthopaedic Principles ICL Kochi by Dr Hitesh Gopalan
FLOOR REACTION ORTHOSIS
A PIECE OF PLASTIC CAN DO WONDERS IF PROPERLY FITTED
– DR APJ ABDUL KALAM
ORTHOSIS :
AN ORTHOPAEDIC APPLIANCE / DEVICE DESIGNED TO CORRECT , PROTECT , SUPPORT OR ASSIST FUNCTION OF BODY PART
FRO is custom made orthosis made of polypropylene or carbon fibre reinforced polypropylene . It is used in quadriceps weakness.
Synonyms : Floor reaction orthosis /Floor reaction ankle foot orthosis / Ground reaction orthosis / Ground reaction force ankle foot orthosis .
Introduced by SALTIEL in 1979 , in India it was popularized by Prof P K SETHI and Prof S C LAKKAD in 1983 .
Components
• Full toe base (foot plate )in equinus (6 -8 degree plantar flexion)
• Uprights
• Anterior / pretibial/ knee piece
Combination of three components allow the plantarflexion -knee extension couple to occur
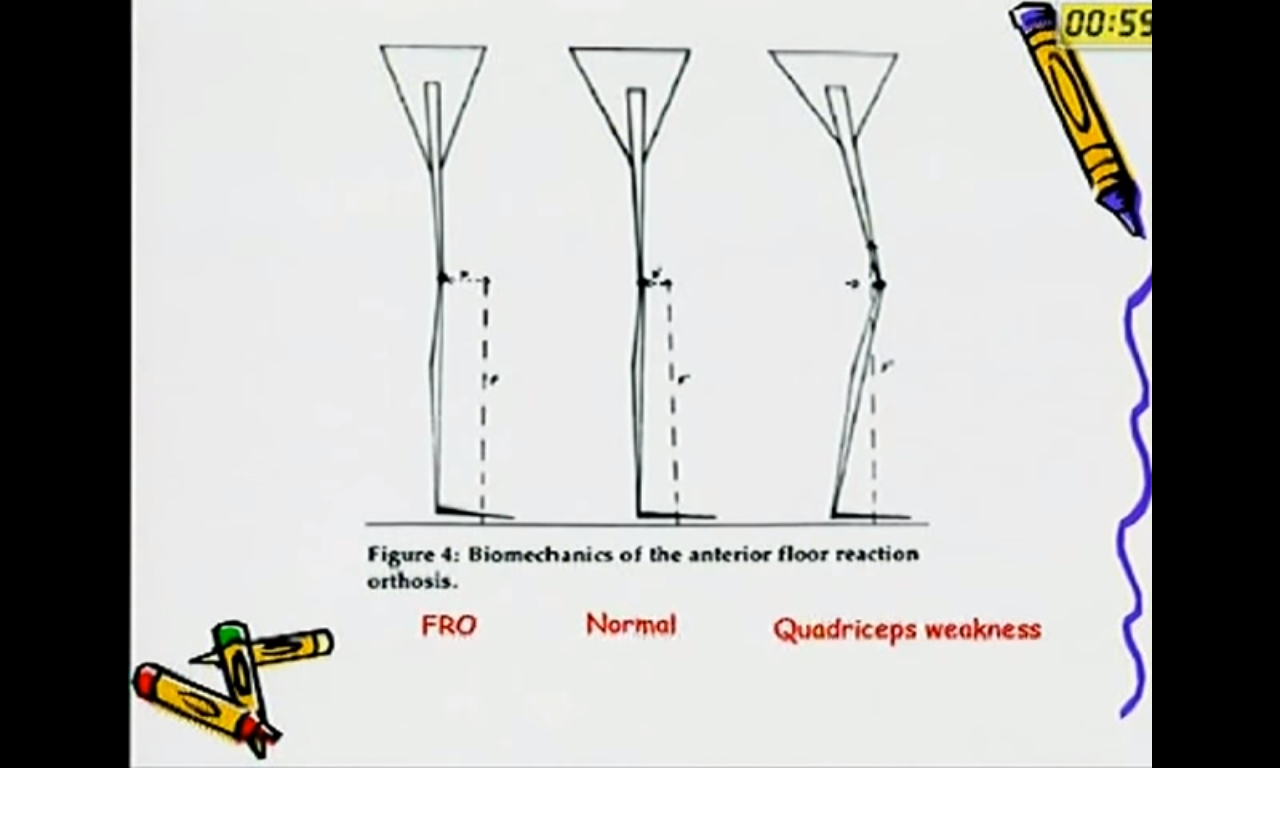
- FRO works in stance phase of normal gait cycle .
- In stance phase the load bearing axis lies in front of the ankle joint , knee joint and behind the hip joint .
- this is possible with the controlled flexion of knee joint and eccentric muscle pull by the quadriceps muscle .
Patient with paralyzed quadriceps , stance phase causes initial contact at heel , weight line to pass posterior to the knee axis , that causes buckling of knee .
Working principle :NEWTONS 3RD LAW
- Initial floor contact occurs at the forefoot as the FRO foot plate made with 5 to 8 degree plantar flexion . this will help the weight bearing axis to pass in front of the knee joint .
- Here the weight of the body over orthosis and over the ground is action.
- foot and orthosis absorb ground reaction forces which enter the body and keep the foot and knee straight .
- During the mid stance phase , the body brings the heel downwards , there is extension moment of prepatellar band pushing the knee backwards, which prevents buckling .
Indications
• Post polio residual paralysis -Most common indication
• Spinal cord injury
• Menigomyelocele
• Cerebral palsy
(Quadriceps weakness )
Wearing schedule : start with one hour on the 1st day and gradually increase with one hour daily , and by 2 to 3 weeks patient will be very much trained to use the FRO.
Usually it is worn over a stockinet or socks to prevent skin maceration. Patient can also wear shoes over the orthosis .
FRO works as a KAFO without a mechanical knee joint .
Patient can utilize his anatomical knee joint without buckling .
Highly complaint /cosmetically acceptable as it can be worn under shoes .
Disadvantages : custom made , skin irritations .
Limitations:
o Hip and knee FFD more than 10 degrees.
o Flail knee / flail ankle
o Angular deformities of foot , ankle , tibia , trunk imbalance .
o Minimum quadriceps strength of 2 +/3 –
Working tips :-
- Avoid using FRO with different shoes , as varied heel height affects stability .
- Ensure heel is properly seated inside orthosis
- Don’t immerse FRO inside water , just wipe dry .


Leave a Reply