Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Flexor Tendon Injuries – Treatment & Rehabilitation
Overview
- Flexor tendon injuries require:
- Early diagnosis
- Timely repair
- Structured rehabilitation
Goals of treatment:
- Restore tendon gliding
- Preserve finger motion
- Recover hand function
Successful outcomes depend on:
- Strong repair technique
- Protection of repair
- Supervised hand therapy
Timing of Repair
- Repair should be performed as early as possible
- Ideally within 2 weeks of injury
Delayed repair increases risk of:
- Adhesions
- Tendon retraction
- Poor tendon gliding
Zone 2 Flexor Tendon Injuries
Importance
- Zone 2 is the “no man’s land” of flexor tendon surgery
- Tendon gliding is easily compromised
Important principle:
- Repairing only one slip of FDS may improve tendon gliding in selected cases
Partial Tendon Lacerations
>60% Tendon Width
- Usually requires repair
<60% Tendon Width
- Often managed conservatively
If triggering occurs:
- Trim frayed tendon edges
Wide-Awake Tendon Repair
Advantages
Performed under local anesthesia.
Benefits:
- Allows active finger movement during surgery
- Assesses:
- Tendon gliding
- Repair tension
- Gapping
Increasingly popular technique.
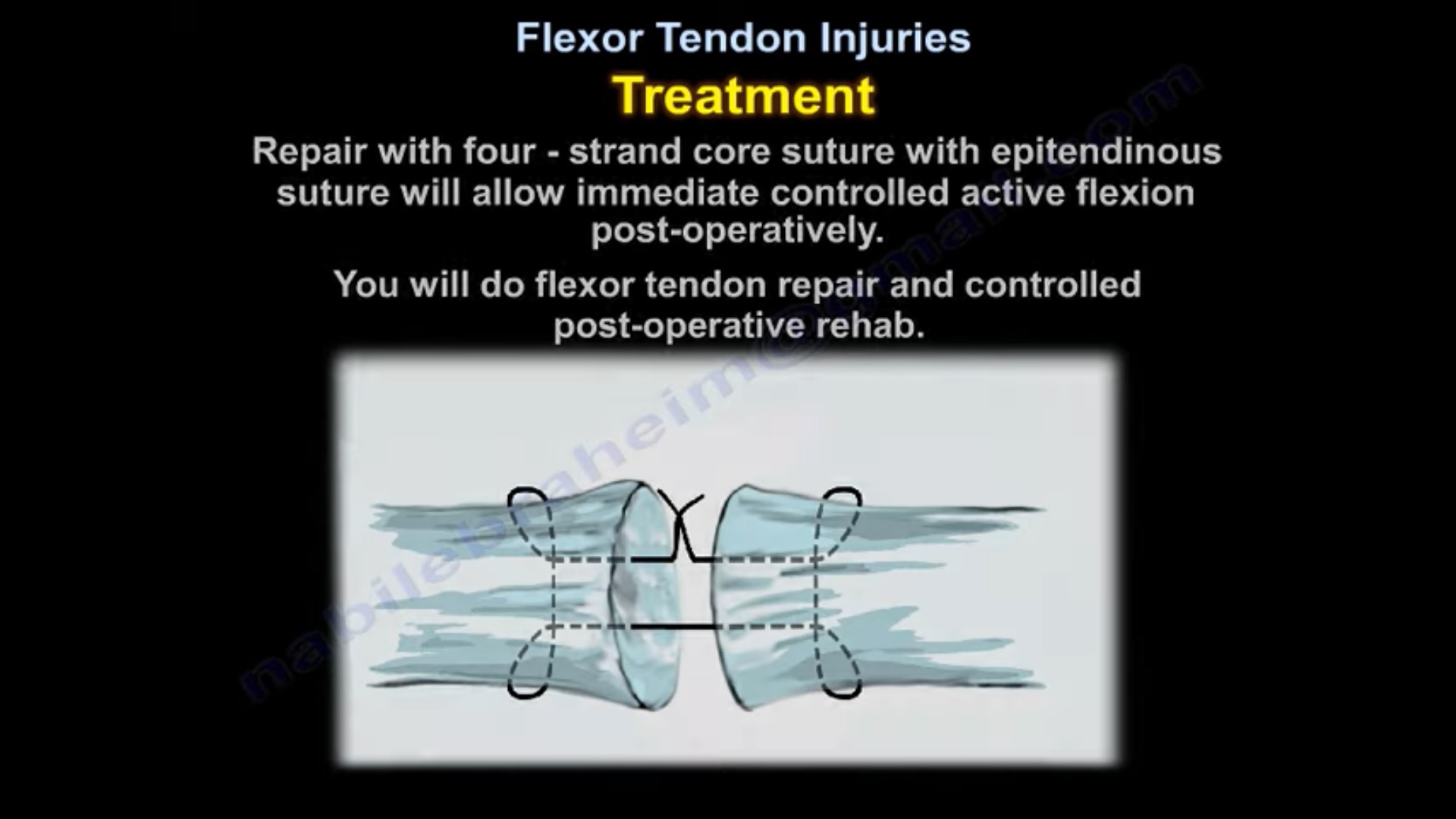
Principles of Flexor Tendon Repair
1. Strong Repair
Repair must allow:
- Early controlled motion
Most important factor:
- Number of core suture strands crossing repair
2. Epitendinous Suture
Benefits:
- Adds repair strength
- Improves tendon handling
- Enhances gliding
3. Avoid Gap Formation
Important point:
- Gap >3 mm increases risk of repair failure
4. Preserve Pulleys
Important pulleys:
- A2 pulley
- A4 pulley
In thumb:
- Preserve pulley system whenever possible
Loss of pulleys causes bowstringing and poor flexion mechanics.
Postoperative Rehabilitation
Importance of Early Therapy
Early controlled motion:
- Reduces adhesions
- Improves tendon excursion
- Improves function
Requires strong repair.
Splint Protection
Dorsal Blocking Splint
Commonly used after repair.
Position:
- Wrist flexion
- MCP flexion
Purpose:
- Reduce tension on repair
- Permit safe controlled motion
Rehabilitation Progression
Early Phase
- Protected passive flexion
Intermediate Phase
- Active ROM gradually introduced
Late Phase
- Resistance exercises after adequate healing
Progression depends on:
- Repair strength
- Rehabilitation protocol
Flexor Tendon Repair in Children
- Young children often treated with cast immobilization for ~4 weeks
- Compliance with therapy may be difficult
Reconstruction of Flexor Tendon Injuries
Indications
- Failed primary repair
- Chronic loss of active flexion
- Preserved passive motion
Single-Stage Reconstruction
Indications:
- Intact tendon sheath
- Good gliding environment
Technique:
- Tendon grafting performed in one stage
Two-Stage Reconstruction
Indications:
- Collapsed tendon sheath
- Poor tendon bed
Procedure:
Stage 1
- Silicone rod placement
Stage 2
- Tendon grafting after pseudosheath formation
Thumb Flexor Tendon Injuries
Flexor Pollicis Longus (FPL) Rupture
May occur after:
- Volar plating of distal radius fracture
Cause:
- Prominent volar plate irritating tendon
Chronic Thumb Flexor Loss
If passive motion preserved:
- Tendon transfer may restore function
Common transfer:
- Flexor digitorum superficialis (FDS) transfer
Important Complications
1. Adhesions
Most common complication.
Especially common in:
- Zone 2 injuries
Features:
- Poor active motion
- Passive motion preserved
2. Tendon Rupture
Highest risk:
- Early postoperative period
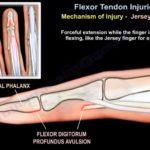
3. Quadriga
Occurs after excessive advancement of FDP tendon.
Leads to:
- Flexion imbalance
- Reduced flexion in adjacent fingers
Important in:
- Jersey finger repair
Tenolysis
Indications
- Passive motion preserved
- Active flexion limited due to adhesions
Initial Management
- Aggressive hand therapy first
Usually wait:
- At least 3 months before considering tenolysis
High-Yield Exam Pearls
- Zone 2 injuries have highest adhesion risk
-
60% partial laceration usually repaired
- Strong repair allows early mobilization
- Gap >3 mm increases rupture risk
- Preserve A2 and A4 pulleys
- Dorsal blocking splint protects repair
- FPL rupture may occur after volar distal radius plating
- Passive ROM preserved + poor active motion = adhesions
- Tenolysis indicated after failed therapy with preserved passive motion
Related Posts
 Flexor Tendon Injuries
Flexor Tendon InjuriesCourtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA Overview Flexor tendon injuries involve trauma…
 Flexor Tendon Injuries
Flexor Tendon InjuriesCourtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
- Revision ACL Reconstruction
Courtesy: Ashok Shyam, IORG, OrthoTV
Leave a Reply