Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Overview
-
Flexor tendon injuries involve trauma to the flexor digitorum superficialis and flexor digitorum profundus tendons.
-
These injuries are commonly caused by lacerations or blunt trauma.
-
They usually result from volar-sided injuries of the hand.
-
Associated neurovascular injuries are common due to close anatomical proximity.
Tendon Healing Mechanisms
Flexor tendon healing occurs through 2 pathways:
Intrinsic Healing
-
Mediated by tenocytes within the tendon.
-
Produces organized collagen and better tendon gliding.
-
Preferred pathway for optimal functional recovery.
Extrinsic Healing
-
Stimulated by surrounding synovial fluid and inflammatory cells.
-
Contributes to scar formation and adhesions.
-
Excessive extrinsic healing leads to restricted tendon motion.
Causes of Flexor Tendon Injuries
-
Sharp cut injuries.
-
Sports-related injuries:
-
Jersey finger
-
Mallet finger
-
-
Rheumatoid arthritis:
-
Rupture of flexor pollicis longus is the most common flexor tendon rupture.
-
-
Attritional rupture due to malunited fractures of the distal radius or metacarpals.
-
Bite injuries:
-
Extensor tendons are more commonly involved, but flexor tendons may also be affected.
-
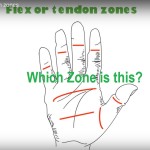
Flexor Zones of the Hand
-
Flexor tendon injuries are classified based on anatomical zones of the hand.
-
Zone-based classification guides prognosis, repair technique, and rehabilitation strategy.
Blood Supply of Flexor Tendons
Synovial Diffusion
-
Occurs when tendons are located within synovial sheaths.
-
Primary source of nutrition distal to the metacarpophalangeal joint.
Direct Vascular Perfusion
-
Supplies tendons outside synovial sheaths.
-
Provided by:
-
Vincular system
-
Osseous insertions
-
Reflected vessels from tendon sheath
-
Longitudinal vessels from the palm
-
Clinical Presentation
Symptoms
-
Loss of active flexion strength.
-
Inability to flex the involved digit or digits.
Physical Examination
Inspection
-
Observe resting posture of the hand and digital cascade.
-
Malalignment or malrotation may indicate an associated fracture.
-
Inspect skin integrity to localize tendon injury.
-
Look for evidence of traumatic joint penetration.
Motion Assessment
-
Passive wrist flexion and extension to assess the tenodesis effect.
-
Normally, wrist extension produces passive flexion of the fingers at:
-
Metacarpophalangeal joints
-
Proximal interphalangeal joints
-
Distal interphalangeal joints
-
-
Persistence of finger extension during wrist extension suggests tendon discontinuity.
-
Active flexion of proximal and distal interphalangeal joints should be tested individually.
Neurovascular Examination
-
Mandatory due to close relationship between flexor tendons and digital neurovascular bundles.
Imaging
-
Radiographs:
-
To identify associated fractures.
-
-
Ultrasonography:
-
Useful for detecting tendon lacerations and discontinuity.
-
Treatment
Nonoperative Management
-
Indicated for partial tendon lacerations involving less than 60% of tendon width.
-
Consists of:
-
Wound care
-
Early controlled range of motion
-
Indications for Tendon Reconstruction
-
Failed primary tendon repair.
-
Chronic untreated flexor tendon injuries.
Flexor Digitorum Superficialis Transfer to the Thumb
-
Single-stage procedure.
-
Indicated for chronic rupture of flexor pollicis longus.
Flexor Tendon Repair
Indications
-
Laceration greater than 75% of tendon width.
-
Laceration between 50% and 60% with triggering.
-
Partial lacerations without triggering can be treated with epitendinous repair alone.
Principles of Flexor Tendon Repair
-
Repair should be performed within 10 to 14 days of injury.
-
Core suture combined with epitendinous suture is recommended.
-
Optimal repair uses 4 to 6 strands.
-
Strickland modification of the Kessler technique is commonly used.
-
Repair sequence:
-
Dorsal epitendinous sutures
-
Core sutures
-
Volar epitendinous sutures
-
-
Minimal gapping at the repair site is essential.
-
Repair failure most commonly occurs at the knot.
-
Circumferential epitendinous sutures:
-
Increase repair strength by up to 50%
-
Reduce gap formation
-
-
Larger suture diameter increases repair strength:
-
Nonabsorbable sutures of size 3 or 4 are preferred.
-
-
Locking suture techniques do not significantly improve repair strength.
-
Wide Awake Local Anesthesia No Tourniquet technique allows real-time assessment of repair integrity.
Timing of Repair
-
Ideal timing is within 2 weeks of injury.
-
Repair should not be delayed beyond 3 weeks.
-
Delayed repair leads to tendon retraction and increased technical difficulty.
Surgical Approach
-
Skin incisions should cross flexion creases transversely or obliquely.
-
Longitudinal incisions should be avoided to prevent contractures.
-
Atraumatic tendon handling is essential to minimize adhesion formation.
Repair Techniques
-
Core tendon sutures.
-
Circumferential epitendinous sutures.
-
Tendon sheath repair when possible.
-
Pulley preservation or reconstruction.
-
Repair of flexor digitorum superficialis when indicated.
Flexor Tendon Reconstruction
Prerequisites
-
Supple skin.
-
Sensate digit.
-
Adequate vascularity.
-
Full passive range of motion of adjacent joints.
Reconstruction Techniques
Single-Stage Reconstruction
-
Indicated when the flexor sheath is intact and digit has full range of motion.
Two-Stage Reconstruction
Hunter–Salisbury Technique
-
Stage 1:
-
Placement of silicone rod to create a pseudosheath.
-
-
Stage 2 (after 3 to 4 months):
-
Removal of silicone rod.
-
Placement of tendon graft through pseudosheath.
-
Pulvertaft weave proximally.
-
End-to-end tendon repair distally.
-
Paneva–Holevich Technique
-
Stage 1:
-
Silicone rod placement.
-
Pulley reconstruction if required.
-
Creation of loop between proximal flexor digitorum superficialis and flexor digitorum profundus stumps in the palm.
-
-
Stage 2:
-
Removal of silicone rod.
-
Proximal flexor digitorum superficialis is divided and advanced distally.
-
Tendon is attached to distal flexor digitorum profundus stump or secured using a button.
-
Graft Selection
-
Palmaris longus tendon (absent in approximately 15% of population).
-
Plantaris tendon (absent in approximately 19%).
-
Extensor digitorum longus to second to fourth toes.
-
Extensor indicis proprius.
-
Flexor digitorum longus to second toe.
-
Flexor digitorum superficialis tendon.
Pulley Reconstruction
-
At least one pulley should be reconstructed proximal and distal to each joint.
-
Pulley reconstruction should be performed before tendon graft placement when reconstruction is planned.
Postoperative Rehabilitation
-
Controlled mobilization is the most important factor in improving outcomes after flexor tendon repair.
-
Especially critical for zone 2 injuries.
-
Benefits include:
-
Improved tendon healing biology
-
Reduced adhesion formation
-
Increased tendon excursion
-
Rehabilitation Protocols
Immobilization
-
Indicated for children and noncompliant patients.
-
Casts or splints position:
-
Wrist and metacarpophalangeal joints in flexion
-
Interphalangeal joints in extension
-
Early Passive Motion
Duran Protocol
-
Low force and low excursion.
-
Active finger extension with patient-assisted passive flexion using static splint.
Kleinert Protocol
-
Low force and low excursion.
-
Active finger extension with dynamic splint-assisted passive flexion.
Mayo Synergistic Splint
-
Low force and high tendon excursion.
-
Incorporates active wrist motion to maximize tendon excursion.
Early Active Motion
-
Moderate force with potentially high excursion.
-
Uses dorsal blocking splint.
-
Includes “place-and-hold” finger exercises.
Complications
-
Tendon adhesions:
-
Most common complication.
-
Higher incidence in zone 2 injuries.
-
Managed with therapy or tenolysis after 4 to 6 months if motion remains restricted.
-
-
Tendon rerupture:
-
Reported rate of 15% to 25%.
-
-
Joint contractures:
-
Occur in up to 17% of cases.
-
-
Swan-neck deformity.
-
Trigger finger.
-
Lumbrical plus finger.
-
Quadrigia effect.

Leave a Reply