Courtesy: Dr Ashok Shyam, Dr. Alvin Crawford, Ortho TV
Pediatric Femoral Neck Fractures
Overview
- Rare injuries accounting for approximately 1% of pediatric orthopedic fractures
- Usually caused by high-energy trauma
- Trivial trauma should raise suspicion for:
- Pathological fracture
- Insufficiency fracture
Common Pathological Causes
- Unicameral bone cyst
- Chondroblastoma
- Osteosarcoma
Epidemiology
- More common in boys
- Incidence in girls is increasing
Delbet Classification
Delbet classification
Type I – Transphyseal Fracture
Features
- Fracture through the proximal femoral physis
- May be associated with hip dislocation
Important Point
- Highest risk of avascular necrosis (AVN)
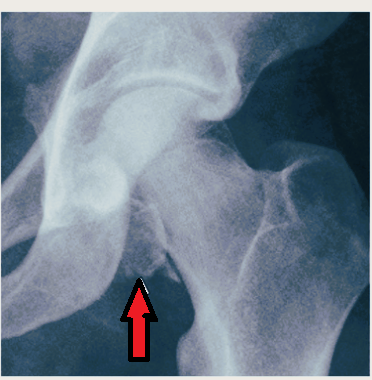
Type II – Transcervical Fracture
Features
- Fracture through the femoral neck
Clinical Importance
- High risk of AVN
- Requires:
- Anatomical reduction
- Stable internal fixation
Type III – Cervicotrochanteric Fracture
Features
- Fracture at the base of the femoral neck
Complications
- Coxa vara
- Non-union
AVN Risk
- Lower than Type I and II
Type IV – Intertrochanteric Fracture
Features
- Best prognosis among Delbet fractures
- Lowest AVN risk
Treatment
- Aggressive fixation still recommended
Type V – Pathological Fracture
Causes
- Unicameral bone cyst
- Chondroblastoma
- Osteosarcoma
Clinical Features
Symptoms
- Severe hip pain
- Inability to bear weight
Limb Position
- External rotation
- Shortening
Differential Diagnosis
Consider:
- Developmental dysplasia of the hip
- Septic arthritis
- Slipped capital femoral epiphysis
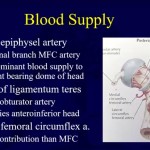
Most Important Complications
1. Avascular Necrosis (AVN)
Avascular necrosis of femoral head
Risk Increases With
- Fracture displacement
- More proximal fracture location
AVN Risk Order
Type I > Type II > Type III > Type IV
2. Coxa Vara
Causes
- Fracture collapse
- Inadequate fixation
3. Non-union
- More common in displaced fractures
- Associated with unstable fixation
4. Premature Physeal Closure
Consequences
- Limb length discrepancy
- Growth disturbance
Note
- Sometimes acceptable if alignment is maintained
5. Chondrolysis
- Progressive cartilage loss and joint stiffness
Management Principles
Pediatric Femoral Neck Fracture Is an Emergency
- Early treatment improves outcome
- Delay increases risk of AVN and complications
Reduction Principles
Goal
- Anatomical reduction
Preferred Sequence
- Closed reduction initially
- Open reduction if anatomical alignment cannot be achieved
Fixation Principles
Stable Internal Fixation Is Essential
Common Fixation Methods
| Age / Fracture Pattern | Fixation |
|---|---|
| Younger children | K-wires |
| Older children | Cannulated screws |
| Basal fractures | Plate fixation |
Additional Technical Points
- Anti-rotation pins improve stability
- Stable fixation prevents redisplacement
- Poor fixation increases complication risk
Capsulotomy / Decompression
Possible Benefits
- Reduces intracapsular pressure
- May decrease risk of AVN
Important Note
- Exact role remains controversial
Important Surgical Principles
- Achieve anatomical reduction
- Ensure rigid fixation
- Prevent rotational instability
- Confirm stable alignment intraoperatively
Counseling Parents
Families should be warned about potential long-term complications:
- AVN
- Limb length discrepancy
- Coxa vara
- Need for future surgery
High-Yield Exam Pearls
- Most important complication: AVN
- Highest AVN risk: Delbet Type I
- Treatment goal:
- Anatomical reduction
- Stable fixation
- Best prognosis: Intertrochanteric fractures (Type IV)
- Trivial trauma should prompt evaluation for pathological fracture
Quick Summary Table
| Delbet Type | Location | AVN Risk | Key Point |
|---|---|---|---|
| I | Transphyseal | Highest | Often associated with dislocation |
| II | Transcervical | High | Requires anatomical fixation |
| III | Cervicotrochanteric | Moderate | Risk of coxa vara |
| IV | Intertrochanteric | Lowest | Best prognosis |
| V | Pathological | Variable | Investigate underlying lesion |
Leave a Reply