Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Overview
-
Femoral neck fractures commonly occur following low-energy trauma in elderly patients, often related to osteoporosis.
-
These patients require thorough medical evaluation and optimization.
-
-
Femoral neck fractures can also occur following high-energy trauma, such as falls from height or motor vehicle accidents.
-
These injuries may affect both younger and older patients.
-
In such cases, management should follow Advanced Trauma Life Support protocols.
-
-
Femoral neck fractures may also result from:
-
Insufficiency fractures, caused by weakened bone due to osteoporosis or osteopenia
-
Stress fractures, caused by repetitive loading and overuse
-
Insufficiency Fractures of the Femoral Neck
-
Occur in patients with poor bone quality.
-
Present with:
-
Groin pain
-
Pain with axial loading
-
-
Initial radiographs may be normal.
-
Magnetic resonance imaging is helpful for diagnosis.
Stress Fractures of the Femoral Neck
-
Occur due to repetitive loading and overuse.
-
Commonly seen in:
-
Athletes
-
Ballet dancers
-
Military recruits
-
-
More frequent in females due to the female athletic triad:
-
Amenorrhea
-
Eating disorders
-
Osteoporosis or osteopenia
-
Anatomic Classification of Femoral Neck Fractures
Femoral neck fractures are classified anatomically as:
-
Subcapital fractures (most common)
-
Transcervical fractures
-
Basicervical fractures
Subcapital Fracture Classifications
Subcapital fractures are further classified using:
-
Garden classification
-
Pauwels classification
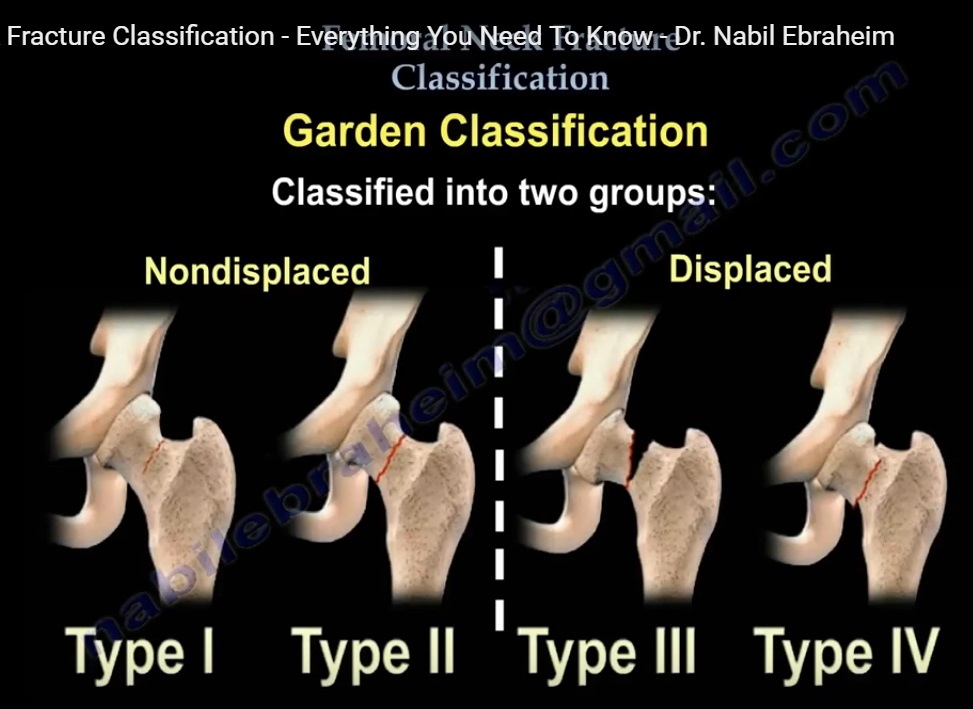
Garden Classification
Principle
-
Based on the degree of fracture displacement.
-
Correlates displacement with the risk of vascular disruption to the femoral head.
-
Most applicable to geriatric and insufficiency fractures.
Groups
-
Non-displaced fractures: Type I and Type II
-
Displaced fractures: Type III and Type IV
Description
-
Type I
-
Incomplete fracture
-
Impacted in valgus
-
-
Type II
-
Complete fracture
-
Non-displaced on both anteroposterior and lateral views
-
-
Type III
-
Complete fracture with partial displacement
-
Trabecular pattern of the femoral head does not align with the acetabular trabeculae
-
-
Type IV
-
Complete fracture with full displacement
-
No continuity between proximal and distal fragments
-
Trabecular pattern of the femoral head remains parallel to the acetabular trabeculae
-
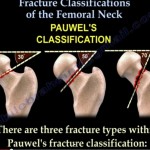
Pauwels Classification
Principle
-
Based on the orientation of the fracture line relative to the horizontal.
-
Reflects biomechanical stability.
-
As fracture obliquity increases, shear forces increase, leading to higher instability and complication rates.
Types
-
Type I
-
Obliquity of 0 to 30 degrees
-
Stable fracture
-
-
Type II
-
Obliquity of 30 to 50 degrees
-
Moderately unstable fracture
-
-
Type III
-
Obliquity of 50 to 70 degrees or more
-
Highly unstable fracture
-
Key Concepts
-
Horizontal fracture lines are more stable.
-
Vertical fracture lines are more unstable.
-
Increasing displacement increases:
-
Risk of vascular disruption
-
Risk of avascular necrosis
-
Risk of nonunion
-
-
Nonunion occurs in approximately 25 percent of displaced femoral neck fractures.
Management of Nonunion in Younger Patients
-
In young patients with nonunion:
-
A subtrochanteric valgus osteotomy may be performed
-
This reorients the fracture line from vertical to horizontal
-
Improves biomechanical stability and fracture healing
-
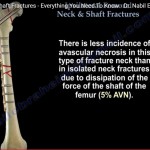
Femoral Neck Fractures Associated with Femoral Shaft Fractures
-
Commonly vertical and non-displaced.
-
May be missed on standard radiographs.
-
Internal rotation views of the hip are often required.
-
Treatment priority:
-
Fixation of the femoral neck fracture
-
Followed by fixation of the femoral shaft fracture
-
-
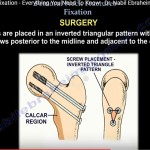
Typical fixation construct:
-
Parallel screws for the femoral neck
-
Retrograde intramedullary nail for the femoral shaft
-
Pipkin Type III Injury
-
Consists of:
-
Fracture of the femoral head
-
Hip dislocation
-
Fracture of the femoral neck
-
-
Closed reduction of the hip dislocation should be avoided when possible.
-
Open reduction of the hip dislocation is preferred, especially when the femoral neck fracture is not displaced.
Classification of Femoral Neck Stress Fractures
A. Tension-Side Stress Fractures
-
Located on the superior aspect of the femoral neck.
-
Adult bone is weak in tension.
-
These fractures are unstable and require surgical fixation.
-
Should be treated as an emergency to prevent displacement.
-
Magnetic resonance imaging is essential for diagnosis.
B. Compression-Side Stress Fractures
-
Located on the inferior aspect of the femoral neck.
Management depends on fracture extent:
-
Less than 50 percent of neck width:
-
Considered stable
-
Managed with protected weight bearing using crutches
-
-
Greater than 50 percent of neck width:
-
Considered unstable
-
Requires open reduction and internal fixation
-
Leave a Reply